| |
March
2018
- Volume 12, Issue 1
Nurses' Medication Errors in the Pediatric Emergency

|
 ( (
|
Manal Fehade
Al- Wahbi Al- Harbi
Correspondence:
Manal Fehade
Al- Wahbi Al- Harbi RN, PhD
Assistant Professor & Chairperson of Maternity &
Child Health Department
Research Center Member at College of Nursing -KSU
Diriyah Female Campus
1st Office. 3rd Flr. Bldg.12
P.O. Box 642, 11421
Riyadh- Saudi Arabia
Tel: +966 118058533
Email: Maalwahbi@ksu.edu.sa;
Manalalharbi7@gmail.com
|
|
|
Abstract
Purpose: Medication errors have been identified
as a major concern in the healthcare industries. The
purpose of the current study was to assess nurses' perceived
contributory factors of medication errors perceptions
on the use medication technology as a strategy to reduce
its occurrence.
Methods: A descriptive
cross-sectional design was used to describe the perception
of nurses and examine their relationship with the profile
characteristics. 200 registered nurses were conveniently
selected from the two of the major tertiary healthcare
facilities in Riyadh which were equipped with pediatric
emergency department.
Findings: This study highlights the significant
role nurses play in the medication administration process.
It has been found out that the 3 top rank factors contributing
to medication errors were interruptions during medication
pass (M= 2.32), shortage of nursing staff (M= 2.13),
and caring for high acuity patients (M= 2.11). Whereas,
hostile work environment (M= 1.56) was the least among
all factors. Moreover, all four types of medication
technologies: barcode medication administration (M=
1.79), computerized physician order entry (M= 1.9),
automated medication dispensing (M= 2.28), and smart
infusion pumps (M= 2.34) were perceived as very helpful
in reducing medication errors. Lastly, the several demographic
characteristics, years of clinical experience (p= 0.01),
and the years of attending pharmacology courses (p=
0.04) were found significantly related with medication
errors. Results of this study have implications for
the staff nurses, hospital administration, and the health
care system in planning for interventions which reduce
medication error and promote establishing of a safety
culture.
Conclusion: Based on the findings of the current
study, a multidisciplinary approach with administration
and research, is needed to solve the problems of medication
errors in the pediatric departments.
Key words: Pediatric nurses, medication, medication
errors, emergency department, patient safety, Saudi
Arabia
|
Clinical relevance
Studies on medication errors are scarce in developing countries,
and the present study was one of the first few relevant studies
which explored medication administration errors in the pediatric
wards in Saudi Arabia. Therefore, the study will ignite awareness
concerning medication safety in Saudi Arabia and also encourage
and ignite interest for future relevant studies. which promote
medication safety.
Introduction
Medication errors (MEs) are the most common type of faults
in the clinical environment. Each year, hospitalized patients
experience 1.5 million preventable MEs related injuries and
hospitals incur an additional $3.5 billion in costs. Several
organizations now support measures to study and improve the
safety of administering medications to promote patient safety
(1) . MEs may be classified according to where they occur
in the medication use cycle, i.e. at the stage of prescribing,
dispensing, or administration of a drug (2) . One of the most
important healthcare workers' last line of defense to protect
against MEs are the nurses. Aside from checking the prescription
and dispensing of drugs which are crucial, nurses ensure the
right calculation, measurement and medication administration.
A study from the nurses in America reported that potential
adverse drug events in pediatric population were three times
more than in adults. Thus, the risk of MEs tend to be higher
in pediatric patients and more likely to lead to serious or
fatal consequences as compared to adults (3) . Among all MEs,
cases involving pediatric patients attract special attention
due to their high incidence and injury rates. The Lan study
reported that insufficient knowledge on pharmacology is the
leading obstacle nurses encountered when administering medications,
which are commonly due to inaccurate doses (4) . Thus, providing
continuing education and double-checking dosages among nurses
is highly recommended(1) .
For healthcare providers working in the emergency departments
(EDs), rapid and accurate measurement of a child's height
and weight upon arrival is critical for accurate medication
dosing (5) . A misplaced decimal point can result in a tenfold
dosing error. In addition, the weights of pediatric patients
can change dramatically, thus frequent recalculation of drug
doses is required. Children are a vulnerable group and have
limited communication skills to warn their healthcare providers
of the adverse effects that they experience. In addition,
all children, especially neonates, have limited internal reserves
that are vital for buffering (6) . The risk of medication
errors tends to be higher in pediatric patients than in adults.
Pediatric dosage of medicine is usually calculated individually
according to the child age, weight, and body surface area
as well as his/ her clinical condition. Even though many errors
are caught before a drug is administered, MEs when not intercepted
by nurses can result in adverse events. Because nurses are
the ones who predominantly administer medications, they are
often the last potential barrier between a medication error
and harm. Nurses must ensure that patients receive the right
medication, right dose, right route, right time and right
evaluation for therapeutic and possible adverse events (6).
Many hospitals have check and balance systems to promote patient
safety during medication administration, however, there are
still possibilities for error. The issues in MEs requires
an examination of the causes and identifying methods for improving
nurse competency and the administration process (7,8). Furthermore,
the process of medication administration takes many steps,
and in any of them, the nurse may commit MEs which are psychologically
devastating to the nurse and harmful to the patient.
Nowadays with different accreditation bodies for hospitals,
attention been given to different aspects of patient safety
including medication administration and medication errors.
MEs have been under-reported in the Middle Eastern regions
including in Saudi Arabia since 1999 (9). Recently, safety
issues in medication administration have started to gain attention
by different nursing scholars and academics. A retrospective
study was conducted among pediatric physicians' medication
orders in Saudi Arabia and results showed MEs occur frequently
with dosage error (10) . Tobaiqy and Stewart's study(11) showed
wrong medications, wrong dose, inappropriate prescribing,
inappropriate route, prescription duplication, and equipment
failure were some of the reported MEs in Saudi Arabia. An
Iranian MEs study identified that the rate of medication errors
was found to be much more than what had been reported by nurses(
12) . Studies on MEs as perceived by nurses are scarce in
developing countries and this present study is just one of
the few studies to be conducted on medication administration
errors by pediatric nurses in the kingdom. Therefore, this
study would serve to ignite awareness and encourage relevant
studies to be conducted in the region. Thus, this study aimed
to describe the factors which contribute to MEs in pediatric
EDs and their perceptions toward the use of medication technology
in reducing medication error.
Methods
Research Design. A descriptive cross sectional approach
was utilized to describe the perception of nurses regarding
MEs, the use of technology for medication administration,
and to establish correlation between variables and the demographic
data of the respondents.
Settings. The study was conducted in the tertiary health care
facilities in Riyadh which were equipped with pediatric EDs.
The selection of the setting was done in two phases: a primary
survey to assess the availability of such pediatric EDs and
the number of working staff nurses. There were 7 hospitals
with pediatric EDs in Riyadh city and only two were selected
based on the number of admissions and number of nurses working
in the pediatric ED.
Subjects. The eligible respondents
passed the following inclusion criteria: (1) working in pediatric
emergency units in Riyadh, (2) experience of ? 3 months (3)
voluntarily participation as respondent. A convenience sampling
technique was utilized since the population was generally
homogeneous, or individual units which were accessible to
the researcher. A power analysis was utilized through Raosoft
Incorporated which was used to calculate the sample size of
200 with an Alpha of .05, power of .80, and effect size of
.50.
Data collection instrument. A
self-administered questionnaire was used for data collection
which was developed by the researchers. Part one of the instrument
focused on demographic characteristics such as gender, age,
nationality, marital status, economic status, highest level
of education, years of clinical experience, time since attending
pharmacology course and their relationship with their family
and with other health care professionals. The other parts
of the questionnaire were designed after reviewing literature
to assess pediatric emergency nurses' perceptions of medication
errors and their barriers to report the medication error.
Therefore, the second part was questions on factors contributing
to MEs and designed after using the Haddon Matrix as a commonly
used matrix in injury prevention to look at factors related
to personal attributes, agent attributes and environmental
attributes; before, during and after an injury(13). These
items were dose calculation, depth of medication knowledge,
interruptions during the medication process, usefulness of
policies and procedures related to medication administration,
nursing workload, patient acuity, overtime hours per day and
week, incomplete medication orders, lack of clinical expertise
in the area one is working, newness to nursing practice, hostile
or tense feelings during medication administration. The third
part were items about the number of medication errors made
by the nurse or a colleague that resulted in harm to a patient
over the past year, or did not harm the patient and evaluated
the number of medication errors that were reported in the
past 12 months including those that caused harm to a patient
and those that did not cause harm. The fourth part of the
instrument assessed technologies used in decreasing MEs. Technology
included in questions were: bar coded medication administration,
computerized physician order entry, automated medication dispensing,
and smart infusion pumps. In part five, eight items were developed
to address pediatric nurses' perceptions for barriers to reporting
(focus on the individual rather than the system, thinking
colleagues will feel the nurse is incompetent, feeling the
error is not important to report, fear of blame, reporting
is time consuming, afraid of a reprimand, afraid of consequences,
and feeling a near miss is not an error). Part six included
factors which might increase the likelihood of medication
error reporting. Seven statements were developed about violation
of any of the "five rights" of medication administration,
anonymous reporting process, safety of the patient has been
compromised, benefits of reporting are identified by nurse,
no fear of retaliation in the workplace, positive relationship
with supervisor, and positive relationship with physicians
the nurse works with on the unit. The last part was about
communication errors and the items were about reporting the
medication error to the patient, or to a family member if
appropriate, and use of medication error report cards. All
scales throughout the survey were developed in closed format
using Likert-type responses utilizing several responses which
included: "Never to Always", "Major Barrier
to Not a Barrier", "Highly Likely to Highly Unlikely",
"Strongly Agree to Strongly Disagree", and "Very
Helpful to Not Helpful.
Validity. Face validity of the instrument was established
via a comprehensive review of the literature in the area of
medication administration errors and was established by reviewing
previously published survey instruments on MEs. To establish
content validity, the questionnaire was sent to an expert
panel (n = 4) of reviewers that had strong expertise in survey
research and medication error knowledge based on their publication
success and minor changes were recommended.
Reliability. A convenience sample of 25 registered nurses
working in the Riyadh area was considered for pilot testing
to test the internal consistency of the items. The instrument
was given to the nurses on two separate occasions. Internal
consistency reliability was tested using Cronbach alpha on
appropriate sections of all returned surveys.
Data Collection Method. After getting the approval
from the selected hospitals' ethical committees, data were
collected between January to June, 2012. Posters, as advertisements
were posted in the units and interested respondents were advised
to contact the researcher. The researcher oriented the respondents
about the objectives of the study, and confidentiality of
their responses and the benefits. Written informed consent
was obtained from each respondent.
Ethical Considerations. Ethical approval was secured
from the Institute Review Board of the university. Confidentiality
of the information obtained was maintained to the best of
the researcher 's ability. The names of the nurse respondents
were not solicited or written down. No record other than informed
consent documents, were kept of the nurse respondents ' identities.
Efforts were taken to minimize the likelihood that any data
could be tied to the identity of any participant.
Data Analysis. Analysis of data was done using SPSS 17.0
statistical software. Descriptive statistics such as frequencies,
range of frequencies, percentages, means, and standard deviations
was used to describe demographic data of respondents. In addition,
independent t-tests, and analysis of variance (ANOVA) was
calculated with appropriate post-hoc tests to determine if
there were significant differences between the means. A significance
level of .05 was used for all of the analysis.
Results
Demographic profile of the respondents. Table 1 shows that
majority were females (93%), belonged to 30-39 age group (41%),
non-Saudi (72.5%), married (66%), in good economic status
(70%), bachelor degree graduate (60.5%), working as a nurse
for >10 years (69%), and (60%) has attended pharmacology
courses for 1-2 years.
Table 1: Demographic profile of
the respondents
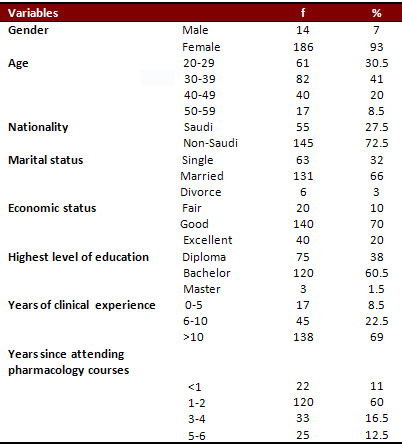
f- frequency, %- percentage
Factors Contributing to MEs.
Table 2 shows that interruption during medication pass (M=
2.32, SD= 0.67) is considered the main factor causing most
medication errors, followed by shortage of nursing staff (M=
2.13, SD= 0.74), and caring for high acuity patients (M=2.11,
SD= 0.73). The least reason to contribute to medication error
is when ED pediatric nurses perceived the working environment
as hostile (M= 1.56, SD= 0.64).
Click here for Table 2: Primary factors of medication errors
as perceived by the nurses
Barriers of reporting and communication of medication errors.
The major barrier for nurses is shown in Table 3. The item
of that the nurse will be blamed got the highest mean (2.83),
followed by that nurses are afraid of the consequences if
they report a medication error with a mean (2.75) and nurses
are afraid of a reprimand if they report a medication error
that had a mean of (2.71). In contrast, nurses think that
Reporting is too detailed and time consuming is a minor barrier
in reporting the medication error as the mean for this item
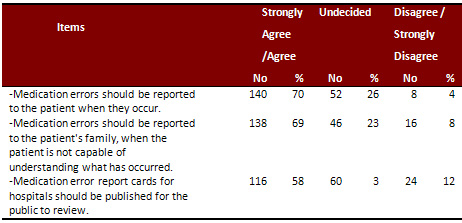
(2.48). For communication of medication errors Table 4 shows
that the majority of nurses overwhelmingly agreed that medication
errors should be communicated to the patient (70.0%). Nurses
also agreed that the patients' family should be notified of
an error when the patient is not capable of understanding
(69.0%). In addition, over one-half (58.0%) of the nurses
surveyed, felt the hospital should publish medication error
report cards for the public to review.
Click here for
Table 3: Perceived Barriers to Reporting Medication Errors
by nurses working at emergency paediatric department
Table 4: Distribution of the sample
according to importance of communication of medication errors
Use of Medication Technology in Reducing Medication Error
Rate
Looking in Table 5, the majority of nurses perceived that
smart infusion pumps (M= 2.34), automated medication dispensing
(M= 2.28), computerized physician order entry (M=1.90), and
barcode medication administration (M= 1.79) all were helpful
in decreasing MEs. In addition, around (20%) to (39%) of the
sample said that most solutions suggested to reduce medication
error, is not available at their hospital.
Click here for
Table 5: Perception of Medication Technology associated with
Decreasing Medication Errors
Relationship between MEs and Demographic
Profile
As shown in Table 6, nationality (p= <0.001, p= 0.001),
economic status (p= 0.02, p< 0.01), and age (p = 0.01,
p=0.01) were significantly correlated to medication error
whether not causing harm or harmed the pediatric patient.
The number of years of clinical experience (p= 0.01), and
years of attending pharmacology course were found to be significantly
(p= 0.04) correlated with MEs which harmed the patients in
the pediatric EDs.
Click here for
Table 6: Chi square test result between relationship with
medication error
Discussion
Several characteristics of the ED nurses were associated with
the MEs which either cause harm or did not cause harm to the
pediatric patients. Similar with the findings, the age of
the ED pediatric nurses has been linked to MEs. According
to Davis (14( , age is an essential factor on how pediatric
nurses closely followed the policies in medication administration.
Age was also found to be significantly correlated with medication
administration errors among nurses coming from 2 regional
hospitals in Riyadh Saudi Arabia(15). The correlation of nationality
to MEs can be attributed to communication errors as non-Saudi
nationals may be caring and giving medications to a Saudi
national patient. In Saudi Arabia nursing care is a mixture
of different nationalities. The cultural diversity of those
nurses implies concern about their ability to communicate
between themselves and with their patients, Alharbi's study
identified that most of the nurses had used another language
to give nursing care due to cultural diversity (16). According
to Albougami(17), current literature
of MEs in Saudi Arabia imply that communication and language
maybe linked. The author added that the errors in health care
service delivery in the kingdom may be attributed to communication
challenges between non-Saudi and Saudi healthcare personnel
as well as between non-Saudi and Saudi patients, however,
the direct effect has not been comprehensively studied. No
scientific literature can support the correlation of the economic
status of the ED pediatric nurses to the probability of committing
MEs. However, this present study identified that most of the
ED nurses with lower salaries are the newly hired or novices
who still lack working experience compared to those with higher
salaries who have been promoted to a higher rank. The economic
status of the ED pediatric nurses is parallel to the length
of working experience. The correlation of years of working
experience and MEs in this study was congruent with the study
of Aboshaiqah(15) with nurses working in Saudi Arabia and
in contrast with the study of Chang which showed that there
was no significant relationship between number of errors and
years of experience for either errors causing harm or "no
harm"(18) .
Nurses need pharmacology knowledge for accurate medication
administration, patient assessment, patient education, and
for some nurses for prescribing; however, less time was spent
in pharmacology education during the college program(19).
Thus, the theory-practice gap leads to a number of identified
anxieties related to insufficient preparation. In a clinical
audit by Morrow-Frost (2006), the more experienced nurses
are more knowledgeable than the nurses with less working experience.
However, the less experienced nurses were more willing to
admit that they cannot provide concrete and correct answers(20)
. Also, new nursing interns and staff nurses have been found
to have poorer mathematical skills than physicians and pharmacists(6)
.
Factors
that are contributing to medication errors
The reasons for MEs among ED pediatrics nurses were similar
to the findings from other studies carried out in USA, Australia
and Turkey. They identify the factors that contribute to errors
such as work load, high patient: nurse ratio causes work-load
time pressure leading to calculation errors and the medication
could not be administrated at the right time. In the present
study, the ED pediatric nurses perceived interruptions as
the topmost reason for MEs. This finding agrees with international
studies wherein pediatric nurses perceived interruptions or
distractions as contributory factors to medications errors
among pediatric patients(21,22). Interruption distracted the
attention of the nurses during the preparation and administration
of the medications and caused calculation errors. Correspondingly
to previous studies, the high nurse to patient ratio and workload
stress renders nurses unable to carry out their professional
role (7) and will more likely contribute to MEs by the ED
pediatric nurses (14,21,22,23,24. In nurse staffing, the high
nurse to patient ratio will consequently lead to increased
workload which commonly occurs in the tertiary health care
facilities in Saudi Arabia. With the chronic shortage of nurses,
the kingdom has been suffering from shortage of nurses and
low production of Saudi nursing graduates with increasing
turnovers of expatriate nurses. Furthermore, the shortage
consequently demands an increasing number of hours by the
other staff nurses as a compromise to staffing issues. Thus,
overtime schedules become prevalent which is a determinant
of burn-out and low work performance which contributes to
MEs among pediatric nurses (25). Also, the finding that high
acuity pediatric cases contribute to MEs was similar to the
finding of Davis(14) which explained that due to the complexity
of cases in pediatric patients, higher incidence of MEs was
noticed compared to than adult patients. Several studies (22,26,27)
showed that the overall experience of pediatric clients who
are sensitive to drug reactions will more likely contribute
to errors.
Barriers of reporting and communication of medication errors
The top three barriers to reporting errors identified in the
current study were: nurses are afraid, the nurses will be
blamed, and a reprimand if they reported medication error.
Thesefindings are congruent with a study(28) which revealed
that fear was found to be barrier for reporting MEs in addition
to knowledge, burden of work, and excusing the error. Another
study(29) identified four major subscales in relation to barriers
to reporting medication errors, which included: disagreement
over whether it was an error, reporting effort, fear, and
administrative response. The barriers identified in the current
study were included under the subscales, fear and administrative
response. As most of the accreditation of healthcare organizations
has required disclosure of adverse outcome as an ethical obligation(30).
In the current study nurses agreed overwhelmingly that medication
errors should be communicated to the patient or to the family
if the patient is not capable of understanding what has occurred.
In addition, the reporting systems dependent on the nurse's
ability to recognize an error has occurred, belief that the
error warrants reporting, belief that she-he has committed
the error, and willingness to overcome the embarrassment and
fear of retaliation for having committed a medication error
(3,31,32). Furthermore, the majority of nurses felt that hospitals
should publish medication error report cards for the public
to review.
Medication technology as helpful in reducing medication
errors
Four interventions with the use of technology that could reduce
MEs were ranked by the ED pediatric nurses. Infusion pumps
ranked first which has been proven to reduce intravenous MEs.
In Pang's study infused drugs with pumps and the frequency
of MEs post-intervention were compared with the MEs in the
pre-intervention period (33). The study concluded that the
use of a specific infusion pump resulted in significant reductions
in the number and clinical significance of intravenous MEs
in administration. Second, the automated dispensing has been
perceived as the least to resolve the MEs in this present
study. Automation dispensing has been shown by James' study(34)
to improve dispensing efficiency and reduce unwanted incidents
which are common during periods of high workload or busy periods,
which were attributed to fatigue among staffs. Third among
the ranked is the use of computer systems. In a review study(35)
the computer systems were reviewed as the most commonly used
intervention to minimize MEs among pediatric and neonatal
patients. The review showed that the ME rates decreased after
a Clinical Decision Support System (CDSS) is used with a Computerized
Physician Order Entry (CPOE). Lastly, Barcode medication administration
(BCMA) system which was perceived as the least to resolve
MEs was shown to be effective in the reduction of MEs (36).
The study used prospective, observational, cohort study of
a BCMA as a tool to reduce MEs and adverse drug events in
a neonatal intensive care unit. Results showed that the intervention
significantly reduced ADEs, controlled MEs, and the associated
risks. The use of technology has been implicated as solution
to a faster and accurate way of delivering healthcare services(37,38).
The review of the literature on safety systems demonstrated
the use of medication administration technology showed that
no particular safety system or practice has been identified
as best to prevent MEs. However, information technology interventions
have great potential for reducing the frequency of errors.
The magnitude of the benefits may be even greater in pediatrics
than in adult medicine because of the need for weight-based
dosing (39,40).
Although the current study contributed to the gap in the literature
by describing the surveyed nurses' perceptions at one point
in time, it was limited by its essence as a descriptive study
that only described various aspects of the MEs (phenomena).
Another limitation is the fact that external factors such
as training and each nurse's work environment were not reviewed.
Some nurses may have had a better orientation and training
experience, leading them to perceive that different factors
impact medication administration errors than their cohorts
with the same amount of ED experience. The study could be
influenced by subjectivity as the researchers developed the
questionnaires which limited the participant's answers. This
study was limited to Saudi Arabia, which could have influenced
the results. A final limitation may be that the surveyed nurses
represent numerous EDs.
Conclusions
The results of the current study have implications for patient
well-being and how to minimize MEs. Based on the findings,
a multidisciplinary approach between the organization and
research is needed to solve the problems of MEs among pediatric
nurses working in the emergency pediatric units. In the clinical
environment, institutional responsibility to prepare and implement
educational strategies and the system can be strengthened
by embedding training from orientation and continuing at all
levels to meet the needs of the nurses. A quality review system
to review drug use and MEs, and implementing computerized
physician order entry (CPOE) or other technological innovations
which is recommended by the American Academy of Pediatrics
be implemented to reduce errors. An integrative approach such
as increased communication through education forums, the presence
of a clinical pharmacist as a team leader and no-punitive
approach by medical and nursing leadership could be alternative
changes that can positively affect patient outcomes. For future
studies, identifying types of interruptions which may cause
MEs and strategies to decrease errors to be used during medication
preparation and administration, is recommended.
References
1- Hughes R, Ortiz E. Medication errors; Why they happen and
how they can be prevented? American Journal of Nursing. 2005;
105 (3), 14-24.
2- Aspden P, Wolcott J, Bootman, J & Cronenwatt R. Preventing
medication errors: Quality chasm series. 2007; Washington
DC: National Academies Press.
3- Chua S, Chua H, et al. Drug administration errors in pediatric
wards: A direct observation approach. European Journal of
Pediatrics. 2010; 169(5), 603-611.
4- Lan Y, Wang K, Yu S , Chen J, Wu F, Tang F. Medication
errors in pediatric nursing: Assessment of nurses' knowledge
and analysis of the consequences of errors. Nurse Education
Today.2013; 821 - 828.
5- Berg B, Cannon-Davis J, Foley A. Pediatric Emergencies:
Preparing at Triage Using Height and Weight. Journal of Emergency
Nursing, 2013; 409-411.
6- Hughes RG, Edgerton EA. Reducing pediatric medication errors:
children are especially at risk for medication errors. American
Journal of Nursing. 2005; 79-80, 82, 85.
7- Antonow J, Smith A, Silver P. Medication error reporting:
A survey of nursing staff. Journal of Nursing Care Quality.
2002; 15(1):42-8.
8- Mayo A, Duncan D. Nurse perceptions of medication errors:
What we need to know for patient safety. Journal of Nursing
Care Quality, 2004; 19(3), 209-217.
9- Osborne J, Blais K, Hayes J. Nurses' perceptions: When
is it a medication error? Journal of Nursing Administration.
1999; 29, 33-38
10- Aljeraisy M, Alanazi M, Abolfotouh M. Medication prescribing
errors in a pediatric inpatient tertiary care setting in Saudi
Arabia. BMC Research Notes. 2011; 4:294
11- Tobaiqy M, Stewart D. Exploring health professionals'
experiences of medication errors in Saudi Arabia. International
Journal of Clinical Pharmacy. 2013; 542-545.
12- Bayazidi S, Zarezadeh Y, Zamanzadeh V, & Parvan K.
Medication Error Reporting Rate and its Barriers and Facilitators
among Nurses. Journal of Caring Sciences, 2012; 1(4), 231-236.
http://doi.org/10.5681/jcs.2012.032.
13- Haddon W. "The changing approach to the epidemiology,
prevention, and amelioration of trauma: the transition to
approaches etiologically rather than descriptively based".
Inj. Prev. 1999; 5 (3): 231-5. PMC 1730511?. PMID 10518273.
doi:10.1136/ip.5.3.231
14- Davis L, Ware R, McCann D, Keogh S, Watson K. Evaluation
of contextual influences on the medication administration
practice of pediatric nurses. Journal of Advanced Nursing.
2009; 65 (6), 1293-1299.
15- Aboshaiqah A. Nurses' Perception of Medication Administration
Errors. American Journal of Nursing Research. 2014; 2 (4),
63-67.
16- Alharbi M.F. Understanding the cultural competence of
nurses in tertiary care settings within the western province
of the kingdom of Saudi Arabia (Doctoral dissertation) 2015.
Retrieved from http://ethos.bl.uk/OrderDetails.do?did=1&uin=uk.bl.ethos.667755
17- Albougami A. Role of language and communication in providing
quality healthcare by expatriate nurses in Saudi Arabia. Journal
of Health Specialties. 2005; 3 (3)
18- Chang Y, Antecedents of severe and non-severe medication
errors. School of Nursing, University of North Carolina. 2009.
Chapel Hill.
19- King R. Nurses' perceptions of their pharmacology educational
needs. Journal of Advanced Nursing.2004; 45(4), 392-400.
20- Morrow-Frost C. Nurses' Knowledge of commonly used drugs:
A clinical audit. Emergency Nurse. 2006; 13 (10), 32- 37.
21- Murphy M. and While A. Medication administration practices
among children's nurses: a survey. British Journal of Nursing.
2012; 21 (15), 928-933.
22- Özkan S, Kocaman G, Özturk C, Seren S. Frequency
of pediatric medication administration errors and contributing
factors. Journal of Nursing Care Quality. 2012; 26 (2), 136-143.
23- Oshikoya K, Oreagba I, Ogunleye O, Senbanjo I, MacEbong
G, Olayemi S. Medication administration errors among paediatric
nurses in Lagos public hospitals: an opinion survey. International
Journal of Risk and Safety in Medicine. 2013; 25 (2), 67-78.
24- Mahmood A, Chaudhury H, Valente M. Nurses' perceptions
of how physical environment affects medication errors in acute
settings. Journal of Applied Nursing Research. 2011; 24, 229-
237.
25- Sears K, Goodman W. Risk factors for increased severity
of pediatric medication administration errors. Healthcare
Policy. 2012; 8 (1) e109-e126.
26- Brady M, Malone A, Fleming S. A literature review if the
individual and system factors that contribute to medication
errors in nursing practice. Journal of Nursing Management.
2009; 17(6):679-97. doi: 10.1111/j.1365-2834.2009.00995.x.
27- Reason J. Managing risks of organizational accidents.
Brooksfield. 2008; Ashgate Publishing.
28- Haw C, Stubbs J, Dickens L. Barriers to the reporting
of medication administration errors and near misses: an interview
study of nurses at a psychiatric hospital. J Psychiatr Ment
Health Nurs, 2014; 21: 797-805. doi:10.1111/jpm.12143
29- Wakefield D, Wakefield B, Uden-Holman T, Borders T, Blegen
M, & Vaughn T. Understanding why medication administration
errors may not be reported. American Journal of Medical Quality
1999; 14(2), 81-88.
30- Covell C, Ritchie J. Nurses' responses to medication errors:
suggestions for the development of organizational strategies
to improve reporting. J. Nurs. Care Qual,2009; 24:287-297.
31- Gonzales K. Medication administration errors and the pediatric
population: A systematic search of the literature. Journal
of Pediatric Nursing. 2010; 25,555-565.
32- Aboshaiqah A. Barriers in reporting medication administration
errors as perceived by nurses in Saudi Arabia. Middle-East
J. 2013; 17:130-6.
33- Pang R, Kong D, de Clifford J, Lam S, Leung B. Smart Infusion
Pumps Reduce Intravenous Medication Administration Errors
at an Australian Teaching Hospital. Journal of Pharmacy Practice
and Research. 2011; 41(3), 192-195.
34- James L.K, Barlow D, Bithell A, Hiom S, Lord S, Pollard
M et al. The impact of automation on workload and dispensing
errors in a hospital pharmacy. International Journal of Pharmacy
Practice. 2012; 21 (2), 92-104.
35- Alsulami Z, Conroy S, Choonara I. Medication errors in
the Middle East countries: A systematic review of the literature.
European Journal of Clinical Pharmacology. 2012; 995-1008.
36- Morriss F, Abramowitz P, Nelson S, Milavetz G, Michael
S, Gordon S. Effectiveness of a barcode medication administration
system in reducing preventable adverse drug events in a neonatal
intensive care unit: a prospective cohort study. Journal of
Pediatrics. 2009; 154, 363-368
37- Talal A. Nurse perceptions regarding
medication administration errors in Hail region hospitals
of Saudi Arabia. Journal of Infection and Public Health. 2015;
8 (4),
38- Chedoe I, Molendijk H, Hospes W, Van den Heuvel, E. and
Taxis K. The effect of a multifaceted educational intervention
on medication preparation and administration errors in neonatal
intensive care. Archives of Disease in Childhood: Fetal and
Neonatal Edition. 2012; 97 (6). 449-455.
39- Kaushal R, Bates D.W, Landrigan D, McKenna K, Clapp M,
Federico F et al. Medication errors and adverse drug events
in pediatric hospitals inpatient. Journal of American Medical
Association. 2001; 285 (16), 2114-2120.
40- Kuperman G, Bobb A, Payne T, Avery a, Gandhi T, Burns
G. Medications-related Clinical Decision Support in Computerized
Provider Order Entry System: A review. Journal of American
Medical Information Association. 2007; 14(1), 29-40.
|
 |

