| |
June
2014
- Volume 8, Issue 3
Phases of Therapeutic
relationship Implementation among the Queen Alia Heart Center
Nurses

|
 ( (
|
Ala'a AL-A'araj
Ahmad AL- Omari
Correspondence:
Ahmad Kamel AL-Omari
Instructor & Faculty Member, Royal Medical Services
College for Allied Health Professions, Department of
Nursing
Jordanian Royal Medical Services
PO box. 36033 , Alhashmy Aljanoubi , Amman , Jordan
11120
Telephone: 00962772080776
Email: ahmadalomari85@hotmail.com
|
|
Introduction
Achieving a relationship of mutual trust and respect between
the nurse and the patient requires the ability to communicate
a sincere interest in the patient (1). The therapeutic relationship
is purposeful and goal oriented, which creates a beneficial
outcome for the patient (2+3), unlike the social relationship,
where there may not be a specific purpose or direction (11+12).
In fact, for interventions to be successful with clients in
all nursing specialties, it is crucial to build a therapeutic
relationship. So, crucial phases are involved in establishing
a therapeutic nurse-patient relationship and the communication
within it which serves as the underpinning for treatment and
success (2+4+10).
The concept of therapeutic relationship
is used in many disciplines and is recognized as one of the
important concepts in nursing (2+3+4+6+9). In the practice,
the therapeutic relationship can be described in terms of
four sequential phases, each characterized by identifiable
tasks and skills, and theses phases are: preinteraction phase,
introduction phase, working phase, and termination phase (2+4+5).
So, the therapeutic relationship must progress through the
stages in succession because each builds on the one before.
In fact, even though most healthcare professionals, including
nurses, know the phases and its skills very well, they have
trouble applying them to their behaviors, particularly in
hospitals where there are a huge number of patients in comparison
with small number of nurses assigned to the patients (3+5+6+7+8).
This gap between the therapeutic
relationship perception and the therapeutic relationship practice
directs us toward this study (5+11+12). So, the purpose of
this study is to assess the current practices and problems
that are encountered regarding the implementation of therapeutic
relationship phases among registered nurses at Queen Alia
Heart Center.
Methodology
The descriptive design was used for this study. A convenience
sample of 200 registered nurses was selected from both genders
with different experiences, who were working in the wards
and units of the Queen Alia Heart Center (Table 1).
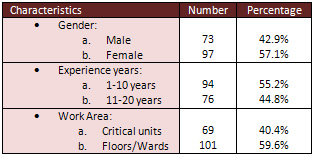
Table 1: The characteristics of the sample
A questionnaire was developed by the researchers and consists
of 25 statements that assessed the implementation of the therapeutic
relationship phases by nurses, in addition to the barriers
for providing the phases according to the nurses. The four
point's Likert scale questionnaire was reviewed by an expert
panel consisting of nurse educator, nurse administrator and
senior nurse colleague to establish its content validity.
The stability reliability was checked by administering the
questionnaire to a group of 40 registered nurses selected
conveniently from both genders with different experiences.
Then after 3 weeks, the same instrument was administered to
the same group. The correlation coefficients were calculated,
and it was equal to (+0.83).
The data collection was carried out on 21 st of July 2013.
The response rate was 85% (n=170).
Results
The therapeutic relationship in our study was divided
into four sequential phases: preinteraction phase, introduction
phase, working phase, and termination phase. The preinteraction
phase involves preparation for the first encounter with the
client, which includes obtaining available information about
the client from the available sources; like their file, family,
and other health team members(2+4+5). The preinteraction phase
also includes examining the client's feeling, fears, and anxieties
before the interaction with the client(10). In our study,
the majority of the nurses either always (46%) or usually
(40.1%) practice the preinteraction phase during their encounter
with their clients, while (10.3%) rarely do it, and (3.6%)
not at all. (Table 2)
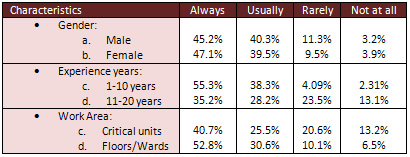
Table 2: The results of preinteraction phase
The second phase of the therapeutic relationship is the introduction
phase. During this phase, the nurse and client become acquainted
(2). This phase includes creating an environment for establishment
of trust and rapport, identifying the client's strength and
limitations, and exploring feelings of both client and nurse
(2+4+5). The introduction phase also includes formulating
nursing diagnosis, setting mutually agreeable goals, in addition
to developing a realistic plan of action to meet the established
goals (4+5+9). In our study, almost three quarters of the
nurses stated that they were either always (32.4%) or usually
(38.5%) practicing the introduction phase of the therapeutic
relationship, while (20.1%) rarely did it, and (9% ) not at
all. (Table 3)
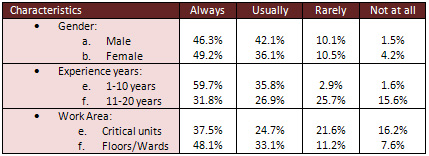
Table 3: The results of introduction phase
The third phase of the therapeutic relationship is the working
phase, in which the therapeutic work of the relationship is
accomplished (4+7+9). This phase includes problem solving
and overcoming client's resistance, in addition to maintaining
the trust and rapport that was established during the introduction
phase (2+5). The working phase also includes continuously
evaluating progress toward goal attainment by using direct
and purposeful questions during the interaction with the client,
while keeping eye contact with them (4). In our study, the
majority of the sample either always (32.8%) or usually (41.8%)
practice the working phase of therapeutic relationship, while
(19.7%) of the nurses stated that they did it rarely and (5.6%)
not practicing it at all. (Table 4).
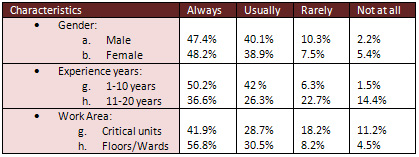
Table 4: The results of working phase
The fourth and last stage is the termination phase, in which
therapeutic conclusions were brought to the communication
and relationship with the client (2+4). This phase includes
attaining of mutually agreed-on goals and setting a plan for
continuing care, in addition to providing health education
according to the client's needs(5). In our study, just one
third of the nurses were either always (13.8%) or usually
(21.2%) practicing the termination phase, while (35.8%) rarely
did and (29.2%) were not practicing the termination phase
at all. (Table 5).
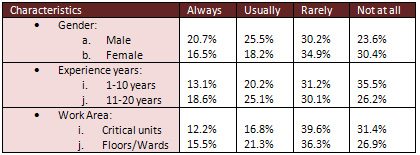
Table 5: The results of termination phase
On the other hand, in response to a question about the biggest
perceived barrier to practicing therapeutic relationship phases
with their clients; 40% of the nurses think that the most
common barrier is gender differences, while 35.4% of the nurses
think that the nursing shortage and educational background
differences are considered as barriers for the practicing
of the therapeutic relationship phases.
Discussion
Although each phase of the therapeutic relationship is
presented as specific and distinct from each other, there
may be some overlapping of tasks, particularly when the interaction
is limited (4). Even then, there are major tasks and goals
during each phase and the client-nurse relationship must progress
through these phases in succession. So, nurses must identify
and practice these phases to build a healthy therapeutic relationship
with their clients.
In our study, the preinteraction phase, introduction phase,
and working phase were practiced always and usually by the
majority (more than 65%) of the participants, while, the termination
phase was practiced always and usually by just about one third
(35%) of the participants. The small percentage of practicing
the termination phase by the participants in comparison with
the other phases reflects the high need to train nurses about
how to practice the phases of therapeutic relationship, because
the therapeutic relationship must progress through the phases
in succession to build a healthy relationship with the clients.
The termination phase is often expected to be difficult and
filled with ambivalence (2+4), which could be caused by the
feeling of sadness and loss that may be experienced by both
the nurse and the client. However, if the previous phases
have evolved effectively, the client generally has a positive
outlook and feels able to handle problems independently (5).
The results of our study also show that both male and female
participants practice the first three phases of therapeutic
relationship in almost the same percentage, but on the other
hand, the male participants practice the termination phase
more than female participants. This could be caused by the
nature of warm emotions that females have more than males.
In related to years of experience, the results show that the
less experienced nurses (1-10 years) practice the first three
phases of therapeutic communication more than the highly experienced
nurses (11-20 years), which may be because the less experienced
nurses are more restricted by the rules of the hospital, and
their knowledge is fresher than the highly experienced nurses.
In contrast, the results show that termination phases are
practiced by highly experienced nurses more than the less
experienced nurses, because the termination phase is more
difficult to practice than the other phases and needs more
experience in dealing with and building relationships with
clients.
In addition, the results show that the phases of therapeutic
relationship are more practiced in the general floors/wards
than the critical units, which may be caused mostly by the
fact that the consciousness and orientation status of clients
in the critical units are lower than in general floors/wards.
Indeed, consciousness and orientation status of the clients
is considered as an integral element of nurse-client interactions
to build the therapeutic relationship (3).
Furthermore, the barriers of practicing the therapeutic relationship
by nurses in our study were mainly the gender differences
between the nurse and the client, then by the huge workload
that is caused by nursing shortage. In the previous studies,
the barriers were mainly the nursing shortage (4+6+7).
Conclusion and Recommendations
The therapeutic relationship is the foundation on which
nursing care is delivered. So, nurses who practice therapeutic
relationships effectively are better able to initiate change
that promote the health, establish trust relationship with
the patient, and prevent legal problems associated with the
nursing practice. Healthcare institutions must provide effective
training to enhance the therapeutic relationship. Indeed,
we hope that the hospitals will heed the call to improve discretion
for the patients who entrust us with their care.
References
1. Smeltzer, S., & Bare, B. (2003). Brunner and Suddarth's
textbook of medical-surgical nursing (10th edition). Philadelphia:
Lippincott. Chapter 3.pages (35-38).
2. Kozier, B., & Erb, G. (2004). Fundamentals of nursing
(7th edition). New Jersey: Pearson Education. Chapter 24.
Pages (428-442).
3. Annells M. (1996) Hermeneutic phenomenology: philosophical
perspectives and current use in nursing research. Journal
of Advanced Nursing 23, 705-713.
4. Tousand, M. (2005). Essentials of psychiatric mental health
nursing (3rd edition). Philadelphia: F.A. Davis Company. Unit
2, chapter 5. Pages (73-83).
5. Brammer, L.M. (1998). The helping relationship: Process
and skills (4th ed.). Upper Saddle River, NJ: Prentice Hall.
6. Bickley, L. S., & Hoekelman, R. A (1999). Bates' guide
to physical examination and history taking (7th ed.). Philadelphia:
Lippincott Williams & Wilkins.
7. Day, L. J. , & Standard, D. (2006). Developing trust
and connection with patients and their families. Critical
Care Nurse, 19(3), 66-70.
8. Peplau, H.E. (1991). Interpersonal relations in nursing.
New York Springer
9. Raskin, N.J., & Rogers, C.R. (1995). Person- centered
therapy.
10. Adam O. Horvath. The therapeutic relationship: Research
and theory. Psychotherapy Research. Volume 15, Issue 1-2,
2005. pages 3-7
11. Fiedler, Fred E. A comparison of therapeutic relationships
in psychoanalytic, nondirective and Adlerian therapy. Journal
of Consulting Psychology, Vol 14(6), Dec 1950, 436-445.
12. Saltzman, C.; Luctgert, M. J.; Roth, C. H.; Creaser, J.;
Howard, L. Formation of a therapeutic relationship: Experiences
during the initial phase of psychotherapy as predictors of
treatment duration and outcome. Journal of Consulting and
Clinical Psychology, Vol 44(4), Aug 1976, 546-555.
|
 |

