| |
March
2016
- Volume 10, Issue 1
What women have to say about giving birth in Saudi Arabia

|
 ( (
|
Ibtesam
Jahlan (1)
Virginia Plummer (2)
Meredith McIntyre (3)
Salma Moawed (4)
(1) Ibtesam
Jahlan
PhD candidate
MCM RN RM
Monash University/ King Saud University
(2) Plummer, V.,
Associate Professor Nursing Research
RN PhD FACN FACHSM
Monash University
(3) McIntyre, M.,
Director of Education
Coordinator Master of Clinical Midwifery
PhD MEdSt B.AppSc RN RM
Monash University
(4) Moawed, S. Prof. Dr. Salma Moawed
Professor of Maternity & Gynaecological Nursing,
Ph. D., M.Sc.N., B.Sc.N.
King Saud University
Correspondence:
Ibtesam Jahlan
Monash University/King Saud University
Telephone: +61 0421 448 127
Email: ibtesam.o.j@gmail.com
|
|
|
Abstract
Background: Reporting the voices of women giving
birth in KSA in order to inform policy developments
within the Saudi maternity healthcare system is important
to understand what the women want from the service and
how to improve it.
Aim: to explore current birthing services in
KSA from care consumers' perspectives by reporting women's
birthing experiences and voices.
Methods: Within the first 24 hours after giving
birth in one of the three selected public hospitals,
169 women shared their birth experience through their
responses to an open-ended question on a questionnaire
or by contributing in one-to one conversation with the
researcher.
Findings: Thematically analysing 169 written
responses and notes for conversation have produced two
main categories which include themes and a number of
sub-themes. The first and major category is "The
relationship between women and care providers during
birth" which is considered by most women the leading
cause for better and satisfied birth experience if this
relationship is characterised by support, respect, trust,
and empowerment. The second category is "Hospital
rules and policies and childbirth experience" especially
if these policies restrict women's choices and are brought
into action without full explanation to women about
why these policies are active.
Conclusion: Maternity care policy makers in Saudi
Arabia have to consider women's voices in building and
reviewing maternity policies and focus on empowering
childbearing women and ensuring safe motherhood.
Key words: Childbirth,
Maternity services in Saudi Arabia
|
1. Introduction
and Literature Review
Maternity services in the Kingdom of Saudi Arabia (KSA)
have been classed by the World Health Organization (WHO) as
comparable with developing countries (1), concurrently, health
services in KSA are experiencing rapid modernization, economic
growth and diversity (2). Maternity services are also being
influenced by these changes. In order to inform policy developments
within the Saudi maternity healthcare system as part of the
modernisation process it is important to understand what the
women giving birth in KSA say about maternity services.
Australia was one of the first countries to conduct reviews
of maternity services inviting submissions from women who
have been consumers of those services. The review sought women's
opinions, experience and degree of satisfaction experienced
with the model of maternity care they received (3-7). Globally,
scholars used women's birthing experience and their voices
to reflect on maternity services. In Scotland, Sweden, Finland
and the USA, reviews for maternity services were undertaken
by exploring women's and/or health care providers' and policy
makers' views about their experiences within the current maternity
care system (8-11). It was suggested that more effort is required
to improve the information provided to women and the choices
available for women regarding the care they receive during
pregnancy and birth (9). Trusting the system was found to
be a major issue for those women who sought non medicalised
care (10). Women reported feeling dissatisfied with the care
they received despite the fact that they were deemed to have
been provided quality care, as measured by the low perinatal
mortality rates. Lack of choice and loss of personal autonomy
in decision making regarding the care they received was reported
as a major source of dissatisfaction (12, 13).
Maternity research in the Middle East region has been focused
on reporting a number of clinical outcomes such as maternal
and perinatal mortality and morbidity and common birthing
practices in line with the medicalization of birth to reflect
on the quality of the maternity services in these countries.
A number of studies were conducted in Jordan and were considered
to be among the first of their kind in the Middle East reporting
women's childbirth experience. These studies show women's
negative childbirth experience using different quantitative
and qualitative methodologies (14, 15) (16). The lack of inclusion
of women's personal experiences of maternity services evidences
a gap in the literature resulting in limitation of maternity
services review findings for the Middle East area.
The voices of Middle Eastern women until now have been silent
and unreported, excluded from policy decisions related to
quality of maternity care improvement. This situation is at
odds with maternity services reviews and research findings
globally, that sought the views of women, the key stakeholders
of the service when it comes to the quality and safety of
maternity services (11, 12, 16, 17).
This study reports Saudi women's experiences of the maternity
care they received, viewed through the lens of safe motherhood
to provide these women's voices with the opportunity to be
heard and in doing so potentially influence maternity service
policy developments in KSA.
2. Methods
2.1 Research design
This study is part of a large mixed method study that explored
birthing services in KSA from two perspectives, women and
health care professionals. Data was collected using the survey
and interviews techniques to describe birthing services in
Saudi Arabia and how these are viewed by women and maternity
health care providers. This paper addresses the findings of
the qualitative section of the study related to the women,
as consumers of maternity care.
2.2 Study sites and participants
This study took place in three specialised maternity hospitals
located in three main cities in Saudi Arabia; Jeddah, Riyadh,
Ad Dammam. The number of births in each hospital is approximately
6000 births/ year (18). One of the three hospitals has achieved
JCA international accreditation, and offers additional services
to those offered by the other two hospitals and consequently
experiences a strong demand by mothers seeking to give birth
in this hospital. For example, the hospital that had JCA accreditation
provides breast feeding classes and consultation through a
breast feeding specialised clinic which is run by breastfeeding
specialist. The other two hospitals provide routine maternity
care. Ethical approval to conduct the research was obtained
from Monash University Human Research Ethics Committee after
the approval was gained from the three individual participating
maternity hospitals in KSA.
2.3 Data collection
One hundred and thirty seven women shared their experiences
related to the maternity care they received, in response to
an open-ended question on a questionnaire. The questionnaire
results are reported elsewhere.
'Apart from meeting your new baby, and knowing that your baby
had no serious health concerns, and apart from the pain you
had during labour and birth, what was the best and the worse
thing about your recent experience of giving birth?'. The
questionnaires were distributed to all eligible women giving
birth in one of the selected hospitals. Participating women
were aged over 18 years, able to read and write Arabic language,
had given birth within the previous 24 hours and cleared for
discharge from hospital after giving birth to a single / multiple
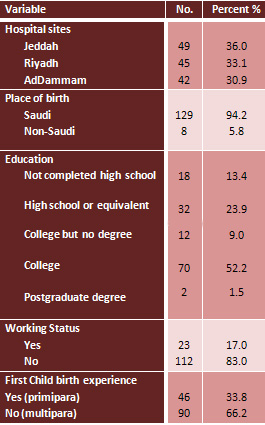
babies (Table 1). The questionnaires were collected in a designated
sealed box at the reception desk in each ward. In addition,
32 of the participating women joined the study through one-to-one
conversation about their last childbirth experience with the
researcher, which was initiated during the distribution and
collection of the questionnaires in the hospital wards. Those
women either were unable or did not wish to write down their
experiences, but wanted to participate in the study. Those
women enjoyed having the opportunity to join the conversations
to share their birth experiences especially when these conversations
took place in a post-natal shared room. Within Saudi culture,
women enjoy speaking to other women of their birthing experiences
as part of an informal debriefing process providing opportunity
to express feelings and fears. This unplanned outcome of this
study (female conversations) enriched the qualitative data
findings with the researcher notes that were written immediately
after each conversation.
Table 1: Participants' Demographics
2.4 Data Analysis
All women's answers for open-ended question and researcher
notes for women's quotes were recorded in Arabic requiring
the data to be translated into English. Following translation
thematic analysis was used to discover patterns hidden within
the texts (19). Thematic analysis began with preparing the
data by transcribing, translating and organizing the documents.
Then the data was explored through reading and re-reading
to a point where the researcher felt totally integrated and
familiar with the participants` words. After that, the researcher
generated initial codes and searched for themes by grouping
the similar descriptions and expressions coded until themes
emerged. Next, the data analysis findings were validated by
reviewing the themes with other research and repeatedly reflecting
to ensure there was no missed classification and that the
identified themes were valid representations of the participants`
perceptions. The final steps were presenting the data analysis
and producing the findings report, wherein the resulting themes
were identified and described using the participants` words
and comments (19, 20).
Rigor was maintained using the golden criteria of trustworthiness
for qualitative research outlined by Guba and Lincoln (21),
which has been applied widely for ensuring the rigor in most
qualitative studies. The criteria, including credibility,
dependability, confirmability and transferability were attained
through reporting the findings by supporting each theme with
women's own words and commentary reflecting women's voices
clearly through each theme. Moreover, sufficient description
for the sample, data collection and analysis is provided for
any possible transferability (22).
3. Results
Thematically analysing women's written responses provided
through returned questionnaires and researcher's notes for
woman-to-woman conversations resulted in a variety of women's
comments that reflect the approach of maternity care delivered
in each hospital. Two main categories of comments evolved
from the data collected regarding what women believed was
the best and the worse things that happened to them during
their experiences of maternity care. A variety of themes and
subthemes have been reported within these two categories.
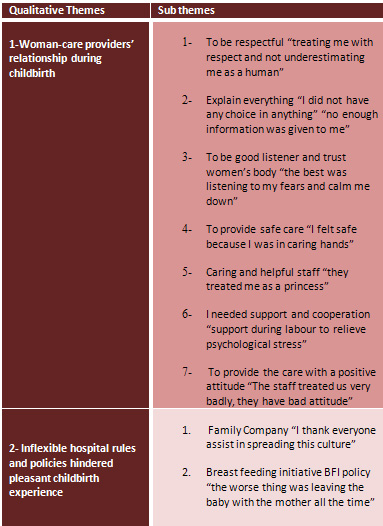
The extracted categories and themes represent women's childbirth
experience in Saudi Arabia. The first and major category is
"the relationship between woman and care providers".
The second category is 'hospital rules and policies and the
childbirth experience'. (Table 2)
Table 2
3.1 The relationship between women and care providers during
childbirth
The relationship between women and care provider is one of
medical domination in Saudi Arabian maternity services where
women are expected to leave all important decisions to the
staff (nurses and doctors) as they are perceived to know best.
The first common experience reported by women relates to the
maternity care providers' support and attitude towards the
women and their respect and interactions with the women. This
category has been divided into seven themes.
3.1.1 To be respectful "treating
me with respect and not underestimating me as a human":
A number of mothers reported appreciation of the staff who
treated them respectfully:
P23: "In the labour and
delivery room the staff treated me very well and with respect.
P134: "the best thing was
treating me with respect and humanity and not underestimating
me as a human".
Conversely, women who were treated with disrespect during
their birth experience expressed their unpleasant feelings
in their words.
P6: "The worse thing was
ignoring me…and not respecting my psychological condition
during labour".
P300: "I felt the difference
between the treatment of the nurse who treats with more respect
than the consultant did."
Similarly, a number of women described feeling embarrassed
by some staff actions that they considered as disrespectful
and humiliating:
P189: "the worse thing
was that during suturing time after birth, the situation was
bad as the Dr.(F) and complete medical team were in the room
which embarrassed me."
C31: "during pushing and
delivering the baby's head, some blood splashed over the doctor.
So, she got angry and said "what brings me here?"
what does she means by that? Why she is working in this area
if it cause her disgust ….."
3.1.2 Explain everything "I did
not have any choice in anything" "not enough information
was given to me":
A number of women expressed their satisfaction with the information
and explanation they received during their last birthing experience.
This was dominated by women who gave birth via caesarean section
because of its surgical requirements and by those who had
previous childbirth experiences.
P51: "as it was a caesarean
section I knew everything".
P173: " the best thing
was knowing the labour and birth stages".
A group of women from the three hospitals expressed their
needs for adequate ante-natal education and during birth explanations
to understand what would be done to them during labour and
birth and why.
P267: "I did not know what
was the injection given with I.V? Also what was the injection
given in my thigh?"
P12: "I did not have any
choice in everything, the midwife left me without dilatation
[episiotomy] till the baby came out without any assistance."
Moreover, women sought for more information during pregnancy
to correct any misconceptions about labour and birth and how
to take care of themselves and their babies after birth.
P273: "when the labour
pain started I had too much of (flower water + saffron) which
increased the pain with no cervical dilatation occurring.
I do not recommend taking anything without a doctor's prescription"
P193: "Not enough information
given to me about my stitches and how to take care of them."
P80: " "I refused
to take a deep breath during pushing because that will draw
the baby water…"
Some women needed more information about their childbirth
experience than others.
P80: "my daughter had the
umbilical cord tied around her neck and I think this is happened
because they did not let me push when I was ready to, is that
true?"
Another group of mothers questioned the presence and the role
of some maternity care providers who attended their labour
and birth.
P11: "I am a human, and
having student trainer during my birth increased my fears.
They should ask for my permission on that."
P309: "the worse thing
was having a male doctor and nurses in my birthing room while
no need for that."
A large number of women have not understood the breastfeeding
policies implemented across a number of the hospitals included
in this study. More antenatal education is required to adequately
prepare women for the change. The main area that women required
more education before the birth was the mechanism of the breastfeeding
and the reasons why breastfeeding was enforced immediately
following the birth.
P100 : "I do not know how
to breast feed my baby and know how to latch my baby to my
breast"
C 10: This woman's son was in
the nursery and she did not know what to do with the milk
accumulated in her breast.
3.1.3 To be good listener and trust
women's body "the best was listening to my fears and
calm me down":
Being cared by someone who listened to women's needs was a
significant factor in a good birthing experience for some
participants:
P279: "the best was the
doctor (F) and the nurse because they were the only two who
listened to my fears and calmed me down during the birth".
Women reported feelings of humiliation because no one listened
to them when they were in labour. For example several women
were very upset and described their experiences:
C31: "I was in pain and
I almost kissed their hands to check me up "sit down
just sit" they said. So I kept bothering them until they
examined me and they found that I was 8 cm dilated."
Then, P80 supports that:
P80: "I felt ready to push,
but the nurse stopped me from pushing and called me a liar.
Then someone came and examined me and saw my baby's head clear
just sitting there."
Another woman described her experience of medical errors as
a consequence of staff not listening to her.
P105: "The decision was
to do caesarean section and they start assessing my sensations
by pinching me and I told them that I felt that but the Dr.(M)
said to me 'you are joking' and I replied 'it is not the time
for jokes, I am in the O.R and I am between life and death'.
So they started cutting the incision and I felt the scalpel
and the stretching; and off course I screamed very loudly.
Then they said fine, fine and they gave me complete anaesthesia".
3.1.4 To provide safe care "I
felt safe because I was in caring hands"
Despite the fact that mothers believed that feeling safe during
labour and birth required a good relationship with the staff
and being informed of the progress, many women did not have
that experience. These women felt unsafe which lead them to
not have a pleasant childbirth experience.
P171: "the best thing was
I gave birth in this hospital which has better care and safety
for patients and informing patients about their rights".
C31: "They documented my
blood type as positive while I am negative, so when I asked
for the injection they told me I do not need it. So, I told
them I had an abortion before in this hospital and I had the
injection. Finally, they did blood test for me. To be honest,
I am very scared about my baby because of the wrong information
they have so they may give my baby the wrong treatment"
Feeling safe for many women was associated with receiving
kindness from their caregiver:
P204: "the best thing occurred
to me during my last birth was the treatment of the health
team with humanity. I felt safe in their hands".
P219: "I felt safe because
I was in caring hands. This was my best birth".
3.1.5 Caring and helpful staff "they
treated me as a princess"
Participating women reported their pleasant childbirth experience
when in the care of helpful, caring staff, and described how
this improved their psychological status and assisted in their
ability to cope with the difficulties of their births:
P120: "the best thing was
the help of the staff during labour and birth."
P134: "The midwife who
took care of me was better than the doctor (F) who I met.
Those midwives knew everything about my condition better than
the doctor herself and they treated it very well, my regards
to them."
Alternatively, one woman who reported receiving good care
also expressed her feelings when encountering uncaring staff.
3.1.6 I needed support and cooperation
"support during labour to relieve psychological stress"
Being cared by supportive cooperative staff was a primary
factor in the mothers' assessment of a better birthing experience:
P298: "the best thing was
the medical team continuous support till the birth complete"
P281: "the medical staff
team in the birthing room were very cooperative and understanding".
Many women reported looking for support and cooperation from
staff and not finding it:
P196: "I waited for 2-3
hours in the waiting area until I could not tolerate the pain
anymore and I was deteriorating physically and psychologically."
P279: "After all this I
have been left in the birthing room till 4 pm without food
or pain killer and with complete ignorance to all my calls
and no kindness".
Experiencing pain is the first characteristic for any birth
experience; a number of women reported their needs for staff
support and cooperation in order to gain control over pain.
P49: "one of the worse
things was the labour pain it was very intense, but it was
treated very well and I was satisfied"
P45: "the worse thing was
the pain and contraction without analgesics."
P12: "….I did not
have any pain relief or oxygen [nitrous oxide]".
Having an induction was not a pleasant experience for some
women and they took the time to express their feelings about
it.
P121: "the worse thing
was being induced in my first birthing experience but then
everything went good with staff help."
Having vaginal examination and episiotomy or stitches are
considered by most Saudi women as a sensitive uncomfortable
procedure and one that increases women's fears and anxiety.
P305: "they agonize us
with vaginal examination."
P146: "My birth was soft,
easy because I did not have any operation or episiotomy".
3.1.7 To provide the care with a positive
attitude "The staff treated us very badly, they have
bad attitude":
Many mothers described what they considered to be bad birth
experiences:
P195: "the worse things
were the nervousness of the nurses and doctor (F)".
P116: "the worse thing
was the treatment by the midwife or nurse. It was bad to the
extent that she told me if you have any problem go out of
the hospital".
C18: "the staff are treating
us very badly, they have a bad attitude"
The experience of being treated badly during labour and birth
affected women's ability to cope. Some women were unable to
overcome this experience:
C28: a woman said after a quiet
period "the doctor treated me badly and kept saying "come
on come on open your legs stop (Dalaa) [this word means acting
like a kid or speaking softly]".
P273: "Everyone I met treated
me with respect except the vaccination nurse, she had a very
bad manner and had religious racism and no kindness".
Several women who experienced staff with bad attitude reported
that this situation prevented them from speaking out for themselves
and their babies.
P89: "after she took the
baby from me she threw him on cot, he was hurt and cried and
I could not say anything because I was tired".
C12: this woman was very upset
because the nurse forced her to breastfeed her twin. "I
was scared and cried as the nurse pinched and hit my thigh
in a funny way to make me breastfeed but I did not like the
way the nurse treated me".
3.2 Hospital rules and policies and childbirth experience:
Childbirth experiences in Saudi Arabia are influenced by what
is offered and allowed in the hospital in which the woman
chooses to give birth. For example, having the husband or
family member attending the birth is not a choice offered
to women in some hospitals in Saudi Arabia. On the other hand,
establishing a new policy such as BFI (Breastfeeding initiation)
required better explanation to women in order to prevent any
misunderstanding or misinterpretation.
3.2.1 Family Company "I thank
everyone who assists in spreading this culture":
For some women having their husband or a family member during
labour and birth was an essential element to improving their
birthing experience.
P11: "the worse thing was
not allowing someone to stay with the patient [woman] although
this is the time when they are desperate to have someone with
them".
P84: "allow husbands of
women to attend the labour, and this should be optional".
P161: ":the best thing
happened during my birth experience and I thank everyone who
assists in spreading this concept which is allowing my husband
to be with me in birthing room, because him being beside me
helped me a lot and made my birth easier."
C24: "They did not allow
my mother until the doctor came and allowed her"
3.2.2 Breast feeding initiative BFI
policy "the worse thing was leaving the baby with the
mother all the time"
Participating women were not happy with the 'rooming in' policy
introduced by the hospital to support and encourage breastfeeding
(BFI). Women expressed their needs for family company during
their hospital stay to help them to take care of the baby.
P49: "I was not expecting
to care of my daughter because I was in a very bad condition,
I was not able to control myself how can I provide care to
my daughter".
P214: "the worse thing
was leaving the baby with the mother all the time, and not
helping the mother changing the baby, because the mother needs
someone to help".
C26: a primi (caesarean section)
woman was so confused and very overwhelmed….She said
"I am very depressed from the pregnancy and birth, I
need someone with me I am primi and gave birth caesarean section".
On the other side, women were unaware that this policy has
been done for a purpose and interpreted this as neglect on
the nurses' behalf. This issue caused an inconvenience for
the women and affected their birthing experiences.
C30: "the important thing
is their limited care to the baby".
P309: "…Also they
did not care of the baby after birth but leaving that to the
mother while she is tired"
P12: "…Nurses refuse
to provide mums with milk for babies although they knew there
is no milk still in their breasts."
P38: "Looking for the nursery
for healthy baby to take them from mothers after birth, so
she can rest for at least three hours".
4. Discussion
Women were willing to share their birth experiences and were
not hesitant to make the most of this opportunity to reflect
on what could be changed to improve experiences for other
women. The relationship between women and maternity care providers
was reported as the dominant factor that influences Saudi
mothers' satisfaction with the maternity care they received.
The most empowering experience for these women was to be cared
for by staff with a positive attitude, someone who provided
continuous support, who showed respect for the person and
who could be trusted to ensure their safety. This finding
has been supported by a number of studies which reported that
positive, trusting and cooperative relationships between women
and maternity care providers were the greatest influence in
women feeling empowered when giving birth (23). The pain associated
with labour and birth can be very difficult experiences for
women who are feeling vulnerable and unsafe. Women's ability
to manage pain during labour is negatively influenced when
feeling unsupported and unsafe (24, 25).
Women reported feeling dissatisfied with their birth experiences
as a result of lacking trust in the maternity care providers
who did not give them the respect they deserved. Respect was
not shown when staff did not provide them with necessary information
on their care and the reasons this care was required, and
or not listening to their needs or ignoring their distress.
This is evidenced when some participating women took the opportunity
to ask the researcher questions about their birth or the condition
of their baby. Educating women regarding what to expect during
pregnancy, labour, birth and breast feeding, and explaining
the role of each member of the maternity care team is a crucial
element in the development of a respectful trusting relationship
which in turn leads to safe maternity care. The need to be
able to trust maternity care providers is closely linked with
the degree of respect that was shown to women by the staff
(25-28).
Having family members to provide support during labour and
birth and post-natally is one of the choices available for
women in most maternity settings within developed countries.
The attendance of family during labour and birth choice was
incorporated into hospitals' policies because of its strong
relationship with the women feeling empowered, in control
of their birth and being more satisfied with their birth experience.
This positive relationship was evidenced by a number of studies
conducted worldwide (25, 27, 29). For Saudi women, it was
a different story as they reported their dissatisfaction and
loss of control as a result of not having the choice to have
a family member attending their labour and birth. Only 22%
of public hospitals in Jeddah one of the biggest cities in
KSA allow a companion to attend labour and birth (2). Nevertheless,
participating women highlighted their needs for family support
through labour and birth as this would help them feel safe,
satisfied and in control. Consequently, women must have the
choice to have a family member throughout their labour and
birth. To do so maternity policies in KSA required some modification
and updating according to women's preferences and latest evidence
regarding having family company during labour and birth.
Moreover, women misunderstood the application of the BFI ten
steps policy as recommended by WHO within public Saudi hospitals
(30). They interpreted the implementation of the policy as
maternity caregiver neglect and carelessness, which was accentuated
in women's words describing their experiences. Having their
babies with them 24 hours and the fact that there is no bottle
feeding provided to babies are the reasons causing women's
misinterpretation and dissatisfaction with birthing experiences.
Changing this policy is not the answer. However, women need
to be informed about this policy early during pregnancy, and
they must be educated why and how the application of this
policy is important (30). This information can be delivered
to pregnant women during antenatal education sessions, which
will prepare them to accept the care delivered to them later
and protect the staff from being misinterpreted.
This study is the first to explore women's birthing experiences
in public hospitals in Saudi Arabia. Women have highlighted
their needs for better, more satisfying birthing experiences.
The overarching need for all women is to be cared for by supportive
cooperative positive maternity care providers who deliver
safe birth care. In addition to the staff support, women were
looking for family support throughout labour and birth as
this is not currently an option for them in most public hospitals
in Saudi Arabia while it was one of the major women's claims.
Furthermore, women showed their demand for more information
about labour and birth, that could be fulfilled with frequent
accessible affordable antenatal educational classes. This
demand also requires continuous explanation and consultation
from the staff during labour and birth. This research sets
off the base for further research reporting Saudi women's
perspectives, voices and experiences regarding maternity care
they receive.
The limitation of this study is that the sample excludes women
who do not read or write Arabic. Also, while this study was
conducted within three large public maternity hospitals that
have high birth rate, this is limiting the representativeness
of the sample of the study.
Conclusion
Maternity care policy makers and maternity care providers
in Saudi Arabia have to consider empowering childbearing women
and ensuring safe motherhood. This can be accomplished by
reviewing and updating maternity policies with women's preferences
and latest up to date research evidence. This study provides
findings that focus on empowering women throughout labour
and birth with the staff and family support, adequate education
and explanation, and availability of choices. The main updates
that this study could add are introducing ante-natal educational
classes during pregnancy, explaining and consulting women
about everything.
Acknowledgements and Disclosures
The authors wish to acknowledge and thank every woman who
spent her time writing or conversing with researcher and sharing
her birthing experience.
References
1. Nigenda G, Langer A, Kuchaisit C, Romero M, Rojas G, Al-Osimy
M, et al. Womens' opinions on antenatal care in developing
countries: results of a study in Cuba, Thailand, Saudi Arabia
and Argentina. BMC Public Health. 2003;3:17.
2. Altaweli RF, McCourt C, Baron M. Childbirth care practices
in public sector facilities in Jeddah, Saudi Arabia: A descriptive
study. Midwifery. 2014;30(7):899-909.
3. Anonymous. QLD:Maternity services review. Australian Nursing
Journal. 2004;12(3):8.
4. Bruinsma F, Brown S, Darcy M-A. Having a baby in Victoria
1989-2000: women's views of public and private models of care.
Australian and New Zealand Journal of Public Health. 2003;27(1):20-6.
5. Brown S, Lumley J. Satisfaction with care in labor and
birth: A survey of 790 Australian women. Birth. 1994;21(1).
6. Bhattacharya S, Tucker J. Maternal Health Services. International
Encyclopedia of Public Health. 2008:210-21.
7. Newnham E. Midwifery directions: the Australian Maternity
services Review. Health Sociology Review. 2010;19(2):245-59.
8. Hundley V, Penney G, Fitzmaurice A, van Teijlingen E, Graham
W. A comparison of data obtained from service providers and
service users to assess the quality of maternity care. Midwifery.
2002;18(2):126-35.
9. Hundley V, Rennie AM, Fitzmaurice A, Graham W, van Teijlingen
E, Penney G. A national survey of women's views of their maternity
care in Scotland. Midwifery. 2000;16(4):303-13.
10. Mander R, Melender H-L. Choice in maternity: rhetoric,
reality and resistance. Midwifery. 2009;25(6):637-48.
11. Ny P, Plantin L, Karlsson ED, Dykes A. Middle Eastern
mothers in Sweden, their experiences of the maternal health
service and their partner's involvement. Reproductive Health.
2007;4(9).
12. Hildingsson I, Thomas JE. Women's perspectives on maternity
services in Sweden: processes, problems, and solutions. Journal
of Midwifery & Women's Health. 2007;52(2):126-33.
13. Miller AC, Shriver TE. Women's childbirth preferences
and practices in the United States. Social Science & Medicine.
2012;75(4):709-16.
14. Oweis A. Jordanian mother's report of their childbirth
experience: Findings from a questionnaire survey. International
Journal of Nursing Practice. 2009;15(6):525-33.
15. Mohammad KI, Alafi KK, Mohammad AI, Gamble J, Creedy D.
Jordanian women's dissatisfaction with childbirth care. International
Nursing Review. 2014;61(2):278-84.
16. Hatamleh R, Shaban IA, Homer C. Evaluating the Experience
of Jordanian Women With Maternity Care Services. Health Care
for Women International. 2012;34(6):499-512.
17. Guest M, Stamp G. South Australian rural women's views
of their pregnancy, birthing and postnatal care. Rural Remote
Health. 2009;9(3):1101.
18. Ministry of Health. Health statistics year book 1432/
2011. In: statistics Gao, editor. 2012.
19. Creswell JW, Plano Clark VL. Designing and Conducting
Mixed Methods Research. Thousand Oaks: Sage Publication; 2007.
20. Braun V, Clarke V. Using thematic analysis in Psychology.
Qualitative Research in Psychology. 2006;3:77-101.
21. Guba E, Lincoln Y. Fourth generation evaluation. London:
Sage; 1989.
22. Prion S, Adamson KA. Making Sense of Methods and Measurement:
Rigor in Qualitative Research. Clinical Simulation in Nursing.
2014;10(2):e107-e8.
23. Goodman P, Mackey M, Tavakoli A. Factors related to childbirth
satisfaction. Journal of Advanced Nursing. 2004;46(2):212-9.
24. Hodnett ED. Pain and women's satisfaction with the experience
of childbirth: a systematic review. American Journal of Obstetrics
and Gynecology. 2002;186(5).
25. Fleming SEMNRNPCNS, Smart DD, Eide PP. Grand Multiparous
Women's Perceptions of Birthing, Nursing Care, and Childbirth
Technology. Journal of Perinatal Education Spring. 2011;20(2):108-17.
26. Goberna-Tricas J, Banus-Gimenez MR, Palacio-Tauste A.
Satisfaction with pregnancy and birth services: the quality
of maternity care services as experienced by women. Midwifery.
2011;27:e231-e7.
27. Corbett CAAMSNFNPc, Callister LCPRNF. Giving Birth: The
Voices of Women in Tamil Nadu, India. MCN, American Journal
of Maternal Child Nursing September/October. 2012;37(5):298-305.
28. Meyer S. Control in childbirth: a concept analysis and
synthesis Journal of Advanced Nursing. 2012;69(1):218-28.
29. Khresheh RRN, Barclay L. The lived experience of Jordanian
women who recieved family support during labor. The American
Journal of Maternal/Child Nursing. 2010;35(1):47-51.
30. Division of child health and development. Evidence for
the ten steps to successful breastfeeding: World Health Organization;
1998.
|
 |

