| March
/ April 2017
- Volume 11, Issue 1
The Future Home Health Care in the Middle East Region:
Part I - International Perspective

|
 ( (
|
Abdulrazak
Abyad
Correspondence:
A. Abyad, MD,
MPH, MBA, DBA, AGSF , AFCHSE
CEO, Abyad Medical Center
Chairman, Middle-East Academy for Medicine of Aging
President, Middle East Association on Age & Alzheimer's
Coordinator, Middle-East Primary Care Research Network
Coordinator, Middle-East Network on Aging
Email: aabyad@cyberia.net.lb
|
|
Abstract
This review is part of a series of papers on home health
care. Home health care has gained widespread acceptance
recently in the developed and developing countries.
This move is affected by the aging of the population,
the improvement in medical technologies and the effort
to improve quality and reduce cost. The home services
vary from nursing care to the concept of hospital at
home. The first part of this paper deals with a general
view of home health care. It presents the American and
Chinese models.
|
Background
A 2011 report by the National Research Council (NRC) in the
USA proclaimed, ""Health care is coming home".
The report additionally noted that in spite of the fact that
the expenses of care are one driver of this change, the conveyance
of services at home is esteemed by people and can advance
well living and prosperity when it is overseen well. Living
autonomously at home is a need for some, particularly people
who are maturing with or into incapacity. However, both the
intricacy and the amount of health care services given in
home settings are expanding.
Also, people with disabilities, interminable
conditions, and functional hindrances require a wide scope
of services and backup to continue living freely. However,
frequently there is not a solid connection between care delivered
in the home and the fundamental social services and back up
for autonomous living. Home healthcare organizations and others
are adapting to present circumstances of taking care of the
necessities and requests of these populations to remain at
home by investigating different models of care and reimbursement
approaches, the best utilization of their workforces, and
advances that can improve autonomous living. These difficulties
and openings prompt the thought of how home services fits
into the future healthcare framework.
Moving
from left to right, Figure 1 demonstrates that this continuum
ranges from look after for lower-acuity levels care to higher
acuity, and from chronic care to more acute care. It additionally
moves from models in which there is almost no physician contribution
in the home toward models in which MD inclusion is significant.
The figure demonstrates that this range begins with casual
care services delivered at home, frequently by relatives-commonly,
daughters, life partners, or daughters-in-law. In the United
States estimates propose that somewhere close to 10 million
and 15 million individuals at present get such care in the
home (Leff et al , 2005).
Figure 1: Home health care across the spectrum of services
and supports, including numbers of individuals receiving care.
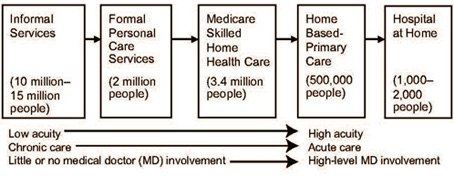
Source: Bruce Leff and Elizabeth Madigan, 2014.
Next, moving right, is formal individual care services-that
is, fees-for services for individuals who require extra help
or who don't have family at home to help them. An expected
2 million Americans get this formal help ( Leff et al 2005).
Next is skilled home health care, which is used for post-acute
care, and in addition for individuals who are homebound, and
have skilled home health care needs. More than 3 million Medicare
recipients use those services.
More to the right is home-based primary
care, which includes doctors, nurse practitioners, or physician
assistants giving longitudinal medical care, which is frequently
group based care and which is regularly given in coordinated
effort by social services suppliers to a population that is
basically homebound. It is projected that at least 500,000
individuals in the United States get these services. Lastly,
on the most distant right of Figure 1-1 are acute care, hospital-level
services delivered in the home, including care delivered through
hospital-at-home-type models, such as the model developed
by the Johns Hopkins Schools of Medicine and Public Health.
To date, Less individuals receive these more intensive home-based
services (Leff et al. 2005).
Leff noticed that the move from left
to right in Figure 1-1 involves a move from the provision
of health care services to individuals with lower-acuity levels
of need to individuals with higher-acuity needs involving
a blend of acute and chronic care services and, lastly, to
provision of acute care in the home. It additionally moves
from models with next to zero doctor inclusion to those in
which contribution is considerable.
The four primary elements driving
the improvement and utilization of this range of-care methodologies
are policy, payment, technology, and demographics. Much consideration
is paid to the last element, as it is expected that we suspect
the maturing of the American population, the anticipated increment
in the quantity of individuals with different multiple chronic
conditions or functional impairments, and the impact that
it's going to have on the health care system, that growth
is a constant, whereas the other elements -policy, payment,
and technology-are amenable to change.
The present array of chronic care
and home-based services is not well coordinated. Patients
may be lost in the system not knowing who is delivering the
services.
In a genuine health care system,
home health care services, would be incorporated into the
mainframe, and those giving these services would deliver care
along a continuum that would include collaborations with partners
in the community as well as those in facility; based long-term
care, because patients often end up there at least for short
periods, before going home again and receiving home health
care services.
Advantages of Home-Based
Care
Home health care offers some essential,
rational points of interest inside the continuum of health
services that are as genuine today. These points of interest
include:
o An upgraded perspective of patients
and parental figures that prompts a superior comprehension
of essential issues, similar to how they oversee solutions
and nourishment;
o Access to medical services that
are most important to patients with physical and financial
hindrances to care;
o A more personal clinician-patient
relationship "around the kitchen table,"
o Clinician articulation of a demonstration
of lowliness that exhibits that clinicians have left their
usual range of familiarity to be on their patients' turf and
that the patient and family merit being really known;
o Lower costs for services that are
sought more by numerous patients;
o And sometimes, more noteworthy
wellbeing for fragile senior citizens, since they will have
less of the basic complexities of hospitalization, for example,
delirium
In view of these points of interest,
the home and community will develop later on as the fundamental
settings for a horde of health care services. The home setting
and health care services and backings will turn out to be
synonymous to the point that they may not be called home care;
rather, they will simply be modern health care.
Home-focused care is fixated on the
patient, offering comprehensive, modern, and individualized
practice to look after individuals with genuine and impairing
conditions. Home-focused care will develop into a noteworthy
national strategy for the arrangement of medical services
since its advantages for both payers and patients are so intense.
Current State of Home
Health Care in the United States
Population patterns are driving the
shape and extent of home healthcare services. Medicare statistics
showed that many people have at least three chronic conditions
(65 percent), half live beneath the destitution line, almost
one third (31 percent) have a psychological or mental impedance,
and around 5 percent live in long-term facilities (Kaiser
Family Foundation, 2014).
Moreover, despite the fact that the
inclination is to bump the Medicare population into one gathering,
around 16 percent of Medicare enrollees are people with inabilities,
more youthful than the age of 65 years and 13 percent are
matured 85 years and older. Notwithstanding these difficulties,
Medicare recipients are regularly in reasonable or weak health,
as indicated by self-evaluations, and have at least two issues
with exercises of everyday living (ADLs).
The development in the span of this
population is contrasted by the numbers of Americans aged
65 years and older in 2002 (35.5 million) and 2012 (43.1 million).
Gauges for 2040 are that somewhere in the range of 80 million
Americans will be age 65 years and older, and around 29 million
of those people will have some level of disability. In the
interim, the quantity of Americans aged 85 years and older
is anticipated to develop from 5.9 million today to around
14.1 million in 2040.
The quantity of organizations giving
home health care in the United States developed from 8,314
in 2005 to 12,613 in 2013, Medicare payments for home healthcare
services almost multiplying from 9.7 billion in 2001 to about
$18.3 billion in 2012. Home health care services constitutes
just around 3 percent of Medicare welfare installments.
The Medicare Home Health Care
Program
Individuals who are perceived as
requiring home health care are the individuals who have had
a current hospitalization or the individuals who have a doctor
referral.
The beneficiary must be under the care of a doctor who has
set up an arrangement of care for the patient (a necessity
over which the home health agency does not have control);
o The care plan must incorporate
the requirement for nursing care or physical, speech, or occupational
therapy;
o The beneficiary must get care through
a Medicare-guaranteed home health organization; and
o The beneficiary must be homebound
and not able to leave the home unaided without the likelihood
of hazard.
Two noteworthy suppositions underlie
these qualification criteria. The doctor drives the care and
the patient has certain necessities (from a clinical point
of view and in light of the fact that he or she is homebound).
Moreover, if a recipient needs talented nursing care, that
care must be required just discontinuously or part time and
must be given by an enlisted nurse (RN) or an authorized practice
nurse regulated by a RN.
Home health aide wellbeing should
complement the care delivered by experts. Extra services that
might be given incorporate restorative social services and
medical supplies. Services that are not secured incorporate
24-hour care, food, and individual care not related with treatment
or nursing. In a few states, in any case, Medicaid covered
these services for low-pay inhabitants prior to the trump
government.
Medicare recipients get talented
care in the home on an intermittent premise. The talented
care look after a specific timeframe-commonly, 60 days-and
skilled care can be reestablished if the recipient needs such
services for a longer time. Conversely, business insurers
back up plans ordinarily approve a specific number of visits
(5 or 10, for instance).
Unskilled services help individuals
securely remain in their own particular home for the longest
timeframe, and in spite of the fact that these services are
not covered by Medicare's home health care services program,
they might be canvassed in different ways or paid for out-of-pocket
that usually is unaffordable. An outstanding model of exhaustive
non institutional care is the Program of All-Inclusive Care
for the Elderly (PACE), a program mutually financed by Medicare
and Medicaid that gives a coordinated arrangement of care
at a PACE center in the community, with some home health services
bolster, for nursing home-qualified beneficiaries.
Quality Measures
National home health care quality
measures assembled for the Centers for Medicare and Medicaid
Services' Home Health Compare site propose that home health
organizations give fantastic services as indicated by key
process measures with home health agencies giving:
o Checks for depression and the danger
of falls 98 percent of the time,
o Instructions to relatives 93 percent
of the time, and
o Timely start of patient care 92
percent of the time.
The normal execution is to some degree
inferior for health outcome measures, which, to a limited
extent, mirrors the debility of individuals who require home
services. For instance, some performance measures show:
o Postsurgical wound care or mending
89 percent of the time,
o Reduction of agony when moving
around 68 percent of the time,
o Improvement in strolling or moving
around 62 percent of the time, and
o Readmission to health care facility
healing center inside 60 days 16 percent of the time.
Overall, the home health care field,
is accomplishing similar readmission rates as hospitals, in
spite of the fact that, the hospital readmission rate is ascertained
just on the premise of readmission in the initial 30 days
after the patient is discharged and, in this way, is to some
degree less demanding to accomplish.
At last, how do recipients themselves
rate the home health care services that they have received?
Once more, utilizing national midpoints from Home Health Compare,
o Seventy-nine percent of patients
say that they would prescribe their home health care services
organization to loved ones;
o Eighty-four percent gave the general
care that they got from the home health care services organization
a rating of 9 or 10 on a 10-point scale;
o Eighty-four percent detailed that
the home health care services team debated solution, torment,
and home wellbeing with them; and
o Eighty-five percent said that the
home health care services group conveyed well.
Reimbursement
Lately, the government has cut Medicare
repayment for home health care services, and sooner rather
than later, another $25 billion "will be removed from
the home health care services framework". Another wellspring
of cuts has come about because of states' moves to oversee
long term care for Medicaid beneficiaries, which has diminished
the quantity of hours of patient care given in the home. Extra
diminishments in business payers' repayments, and in Medicare
Advantage, Medicare's overseen care program, have happened.
More money related difficulties result
from the abnormal state of examination and reviewing to which
home health agencies are subjected, which have been brought
about partly from extortion and mishandling in the system.
Emerging Innovations
Home health care suppliers are included
with various developing models that sort out and pay for care
differently. Among them are developments that were built up
under the Patient Protection and Affordable Care Act of 2010
(ACA), for example, accountable care organizations (ACOs)
and packaged installment plans. In particular:
o Home health care associations are
discovering chances to work specifically with
ACOs to convey community based care.
o Home health care associations are
included with the arrangement of post-intense care benefits
that include the utilization of both home health care and
talented nursing to give the correct level of care after hospitalization.
o Increasingly, home health care
associations are included with transitional care, in which
their first visit to the patient is in the hospital and afterward
they make maybe one visit after the patient is released.
o Home health care associations'
patient appraisal aptitudes and
experience working in the house are being tapped for assessments
of high-hazard enrollees in health plans.
The test is to take care of the expense
of these services extensions. The foundation of home health
agencies has been worked around Medicare, and these new plans
oblige organizations to work in an unexpected way. Everything
from programming frameworks to care conveyance models should
be upgraded, and mentalities should be balanced. Moreover,
rivalry in these rising fields is huge: "Everyone needs
to be in this space at this moment". Coordination among
the different elements giving transitional care-the hospital,
the insurance agency, and others-is not effortlessly accomplished.
For quite a while, despite the fact
that home health care services have tended to utilize electronic
records for both the accumulation of clinical data and survey,
important utilization arrangements under the ACA don't have
any significant bearing on long term care. Home health care
additionally has not profited from the trading of clinical
information with different suppliers, nor do home health agencies
have the patient portals that hospitals are required to give
their patients. Bigger home health organizations are giving
careful consideration to revealing and investigation of quality
outcomes, yet littler ones experience difficulty paying for
information examination and electronic records frameworks.
At long last, telehealth applications
(e.g., video, remote observing, automated calls) have been
observed to be successful and financially savvy by a few associations.
Be that as it may, no extra repayment is accommodating the
improvement and utilization of telehealth, a lack that is
restricting the trend.
Elements for Progress
Four principle elements will be expected
to impact this development and can be set up by all assortments
of payers and associations:
o Development and oversight of interdisciplinary
Home health care arranged by doctors and practice nurse educated
by established ideas of all encompassing geriatric medicine,
palliative solution, and restoration medicine;
o Enhanced care transitions that
tackles self-administration, care coordination, data exchange,
and clinical adjustment;
o A capacity for raising the power
of therapeutic and palliative care at home in times of decreased
or compounding of a patient's disease or restorative condition
(counting acceleration to doctor's facility like administrations
at home); and
o The mindful utilization of cutting edge data innovation
between experiences to help with the administration of issues
that emerge amongst visits and to enhance triage and the general
effectiveness of care.
The absolute most essential issue
is figuring out if the capability of home-focused care is
acknowledged and the pace at which it will be acknowledged
is the quality of the country's Medicare-affirmed home health
organizations. These associations exist in every community;
and utilize a huge number of staff who are attendants, advisors,
different clinicians, and helpers; who make more than 100
million home visits every year; and aggregately, have numerous
solid community ties.
An arrangement of strategies that
would bolster the home medical services foundation and help
it assume the function would
o Tie installments to results and
encounter and encourage supplier interest in an assorted scope
of installment option models;
o Enable the contracting of medical
chiefs (who might, for instance, connect home
health services to the services offered by other key suppliers);
o Have interdisciplinary group case
surveys, like the approach utilized by
hospices;
o Make the mediations utilized amid
the move of care, a secured home health
services benefit, independent of whether a patient is homebound;
o Facilitate innovation to enhance
the stream of data among suppliers
and between home care organizations and the patients and families
served; and
o Advance training and preparation
of professions for organization staff in state-of -the-art
geriatric, palliative, and rehabilitation medicine, and in
procedures for the coordination of care.
This focal part would be further
supported, by making real misrepresentation and mishandling
concerns a relic of past times. Later, home care agencies
ought to certify not exactly at the season of licensure but
rather on a progressing premise. Chosen use measurements ought
to be freely announced. Esteem based acquiring and oversight
models ought to diminish fluctuation crosswise over organizations,
and endeavors ought to be made to weed out less able elements.
In the event that this were done, even the Medicare-guaranteed
home health agency of 2024 with the most minimal level of
execution would be "a genuine and gifted clinical association
with the ability, culture, and innovation [required] to be
a center for some portion of helping doctors and home attendants
addressing Medicare cost and quality difficulties."
The best models and approaches and
the assets and strategies required for achievement will be
recognized after some time. All in all, a brilliant home-focused
health system is plainly and substantially before us on the
off chance that we keep on nurturing the seeds of progress
that are beginning to develop, while finding a way to advance
as opposed to decreasing our home health organizations.
Lessons From Japan and China
In Asia, home health care model needs
to be adapted to locally based on the socioeconomics of the
population and different difficulties.
In China, the size of the population
and the associative difficulties can be difficult to envision.
By 2020, China will spend more than the United States on health
services, despite the fact that they are spending far less
per capita than the United States. One of the difficulties
in managing the maturing population in China is the one-child
family. They now have a normal couple attempting to deal with
four, now and again eight individuals, if the colossal number
of grandparents are alive. Despite a centuries-in length social
convention of obedient devotion and predecessor adoration,
the Chinese government in 2013 joined some different nations
in receiving a law saying that individuals needed to deal
with their maturing guardians' money related and profound
necessities.
China's developing elderly population,
consolidated with its vacillating financial difficulties,
is driving some truly inventive. An approach test that the
Chinese face, as do numerous nations, is the separation of
the medical care and social care parts. The segments need
to join their assets with private family assets to empower
a group to choose in a complete, adaptable manner what an
individual or family needs most. This is as opposed to installment
frameworks that oblige assets to be utilized as a part of
particular ways.
Examination of the quantities of
specialists and nurses in China, particularly those trained
in geriatric care, stacked up against the developing need
shows such a sizable needs, to the point that plainly the
nation can't depend on a doctor and caretaker driven model.
The greater part of these individuals will never at any point
approach a doctor or caretaker in their lifetimes. The nation
should embrace a community health worker-driven approach that
can likewise enroll family individuals and neighbors in some
really concentrated ways. The fate of care is group based,
cooperative, comprehensive, and in the community.
China is presently attempting to
build up a technique concentrated on making a community mind
workforce, foundation, and plan of action. In truth, such
a model can serve individuals of any age, so the contention
for it can be founded on universal design principles. The
model that the Chinese are attempting to construct is "care-flow
service networks " that will permit various organizations
and agencies- government service providers, benefit providers,
service providers, or family-to utilize a typical infra-structure
to convey care in the community and, in the meantime, permit
significant development in the applications utilized and services
provided.
The Chinese are as of now building
savvy stages in view of exercises of regular day to day existence-railroad
utilization, correspondence, shopping, and telephones and
various technology They are not contemplating health services
in segregation, as frequently occurs in the United States,
expecting that "everything else" is some way or
another dealt with. They have as a top priority an entire
social engagement framework that incorporates the services
required for protected and secure living.
Without a doubt, some portion of
the test for the Chinese in outlining this complete administration
framework is managing the scale contrasts from little rustic
settings to medium-sized towns to the current huge urban areas.
Approximately 20 new megacities that will have this old-age-friendly
city foundation set up are being worked without any preparation.
The national government's present 5-year plan includes beginning
these, and by 2020, the Chinese would like to give 90 percent
of care to older individuals in their homes.
Personal Health
In the United States, what business
procedures and development techniques can change the model
of care? By 2017, the US will have more individuals on the
planet who are over 65 than under the age of 5 years old for
the first time in mankind's history. Aging population and
rising health care expenses are concerns around the world.
Numerous nations are "managing the triple point improving
the nature of patient care, enhancing population wellbeing,
and diminishing the general cost of care. They see the requirement
for senior services overwhelming the workforce, delivering
medical services specialist deficiencies and making migration
challenges far and wide.
What they are longing to do is to
"move left," that is, to get more individuals on
the finish of the health continuum with lower levels of chronic
illness, bring down levels of functional impairment, bring
down expenses of health care, and a higher personal satisfaction.
Advancements in policy or innovation
may encourage governments to fulfill the move to one side
in the outline in Figure 1. The relocation of technologies
that help that happen are now happening. This relocation of
technologies brings up huge issues for the United States,
including the accompanying:
o What are the wellbeing and security
suggestions?
o What does this movement mean from
an administrative point of view?
o How can abilities be moved with
the goal that individuals can begin performing errands thought
to be the domain of the general population on the right of
the diagram in Figure 2, in light of the fact that there won't
be sufficient limit on the right?
o How is time moved to the left side in the chart in Figure
2with the goal that preventive care and essential care should
be possible to constrain individuals to right side of the
graph from constantly happening?
Figure 2: Intel strategy for innovation: shifts in place,
skills, and time from the mainframe model to the personal
health model

Figure 2: Intel strategy for innovation: shifts in place,
skills, and time from the mainframe model to the personal
health model.
Health care needs to move also from a health service module
to an individual wellbeing model. Later on, the health services
system won't be maintainable, unless it has a proper framework.
Patients who understand that their clinicians may have different
backgrounds and motives seek second, third, fourth, and fifth
opinions.
The second necessity, is for all
the different body parts and frameworks and for all the cell
level understandings to be reintegrated into entire individual
care. Despite the fact that the advancement of specialty care
has been critical in giving a comprehension of the science
behind wellbeing and disease, experts may turn out to be unexpectedly
one-sided by the medications they prescribe.. Patients who
comprehend that their clinicians may have distinctive foundations
and thought processes may look for second, third, fourth,
and fifth opinions.
The use of huge information examination
to cases information may create more hearty hazard appraisals
at the population level yet may not illuminate the decisions
of an individual patient.
Mainstay of Personal Health
Care customization manages the shift
from population-based to person- based treatment. Although
that includes personalization based on genomics. Early experiments
demonstrated that consistent positive behavior change is possible,
as long as clinicians communicate with people in the way in
which they prefer.
A few movements of the health services
framework that would shore up the three pillars are required.
A few cases incorporate the accompanying:
o Moving from expert care to more
self-care.
Frail elderly: These can give self-care
if the advancements are usable and the advantages (the incentivized
offer) to them are clear. Regardless of the possibility that
lone 20 percent of patients can use self-care, it would move
the needle on cost, quality, and access. That 20 percent of
patients would be the great early adopters, and after some
time, more individuals will have the capacity to move toward
self-care undertakings.
o Moving from exchange based care
to care coordination. Programming apparatuses can encourage
such a move by supporting groups, as said above, and giving
status reports progressively.
o Moving from " medical-ized"
records to "life-ized " ones. Information that is
more extensive than the information that is generally important
to the medical group should be incorporated into the records
for the patient, despite the fact that whether that information
will be incorporated into various information frameworks or
somehow consolidated into a solitary framework still can't
seem to be resolved.
"We need to escape this attitude that all that we have
to do should be costly. They likewise may turn out to be progressively
not so much costly but rather more broadly accessible.
Principles for the Evolution of
Health Care
Instead of an emphasis on technology,
it is recommended to follow a number of
principles that will encourage the advancement of health services
and the already portrayed "move to the left" (see
Figure2):
" Move the place of care to
the minimum prohibitive setting.
" Shift abilities to patients
and parental figures.
" Shift the time of care so
it is proactive and not receptive.
" Shift installments from individual
suppliers to groups of suppliers of care and move installments
so that results that mirror the utilization of a all encompassing
methodology are accomplished.
The beginning stage for these progressions,
is the social covenant that declares, "We as a culture
have concluded this is the manner by which we're going to
set ourselves up for individuals who require care and the
individuals who give it."
Home Health Care Under Medicare
and Medicaid
Currently home health services, the
ordinary storehouses of Medicare and Medicaid do occasionally
cooperate and cover, however they are not really incorporated.
Medicare is an entitlement program that covers Americans aged
65 years and older and people under age 65 years with permanent
disabilities in a uniform way across the country. Medicaid,
by definition, is more complicated because of the combination
of federal requirements and the different eligibility and
benefit rules of each of the 50 states. The low-income people
who are eligible for Medicaid and who receive home health
care services often are also covered under Medicare (and are
referred to as dually eligible), which is their primary coverage.
Home-based services (including nursing
services; home health aides; and supplies, appliances, and
equipment) are obligatory benefits under Medicaid, but the
more extensive cluster of home-and group based administrations
is optional. Even in this way, states may force restrains
on their Medicaid home health services programs. Five US states
have put restraints on program expenses, and 25 states and
the District of Columbia limit benefit hours. The advantage
is commonly secured under fee-for-service arrangements, albeit
many states are moving toward the utilization of capitation.
As in Medicare's home medical services program, a doctor needs
to give a written arrangement of care to beneficiaries to
be qualified for Home health care services.
Obligatory advantages for people
who meet all requirements for Medicaid home medical services
incorporate low maintenance or irregular visits by a registered
nurse; home helper services by credentialed specialists utilized
by participating home health agencies; and fitting therapeutic
hardware, supplies, and apparatuses. Physical, occupational,
and speech therapy in addition to audiology services are discretionary
advantages. Fifteen state Medicaid programs permit beneficiaries
to mastermind their own particular services, including providing
installment to family parental figures. These self-coordinated
administrations programs have for the most part demonstrated
fruitful in diminishing neglected patient needs and enhancing
wellbeing results, personal satisfaction, and beneficiary
fulfillment at a cost comparable to that of customary home
health agency-directed service programs.
In the customary Medicare program,
which utilizes fee-for-service payments, it has been generally
simple to track how much that open protection pays for different
sorts of services, including home medical services. Be that
as it may, as expanding numbers of Medicare and Medicaid beneficiaries
are moving into capitated plans, estimation of the quantity
of individuals receiving services, the amount they are getting,
and what government source is paying for these services gets
to be distinctly harder. Under fee-for-service programs, Medicare
right now pays the biggest share of home medical services
uses (44 percent), even with its generally contract qualification
criteria, trailed by Medicaid (38 percent) Private coverage
and other outsider payers pay around 10 percent, and another
8 percent is paid out-of-pocket. The measure of out-of-pocket
spending is most likely downplayed, in light of the fact that
no solid methods for catching this information exists.
Home medical services remain a generally
little bit of aggregate Medicare and Medicaid spending.
Who Is Served?
Around 66% of all Medicare home health
services clients have at least four or more chronic conditions
or if nothing else, one functional disability. People receiving
home medical services are regularly physically compromised
and cognitively affected. These are individuals with numerous
difficulties. Although the majority of these difficulties
emerge with regards to ageing, they likewise confront the
number of inhabitants in individuals with handicaps secured
by Medicare.
Home health care utilization by and
large, the quantity of home medical services visits per client,
and Medicare spending per client all ascent with age, as does
the utilization of numerous other health care services, including
inpatient care, talented nursing care, and doctor services,
and the utilization of a few medications (yet not hospice
care). The age-per capita spending curve for each of these
services has a peak. For instance, doctor services and outpatient
drug spending top at age 83 years, declining from that point,
and that after age 89 years, hospital expenditure uses begin
to drop. Spending on home health services does not peak until
age 96 years, and spending on skilled nursing facilities tops
at age 98 years.
Albeit just 9 percent of the conventional
(i.e., non-managed care) Medicare population gets home medical
services benefits, the health services spending for these
people represents 38 percent of customary Medicare spending.
Some questions about these patterns of care:
o Are recipients receiving care in
the most fitting setting?
o Are they receiving great quality
care in?
o Does this pattern of care ideally
adjust government, state, and family spending plans?
o How will the country fund care
to an aging population?
In general, the utilization of Home
health care services has expanded as of late, reflecting both
a maturing population and the ascent in the occurrence of
chronic conditions noted before. In any case, spending on
home medical services, which had been rising correspondingly,
has leveled off as of late, despite the fact that home health
services serves more individuals. This might be expected to
some extent to installment decreases from the Patient Protection
and Affordable Care Act of 2010 (ACA)2 and more prominent
late endeavors to address extortion in a few pockets of the
nation.
Trends in Public Policy in the
United States
On a very basic level unsustainable
health services cost direction that the USA is on, Federal
spending shortfalls will develop in respect to the GDP, and
in 10 years, intrigue installments are anticipated to be bigger
than the U.S. Department of Defense spending plan, creating
a tight cash condition.
At the focal point of these troubles,
are the projects that compensation 80 percent of the home
health services charges: Medicare and Medicaid. Medicare is
spending its assets quicker than finance charges and premiums
are recharging them and will go under expanding monetary pressure.
Medicaid faces comparative pressure, particularly at the state
level.
The home health services industry's
money related condition looks particularly problematic, with
somewhere in the range of 40 percent of Home health care suppliers
anticipated that would be in the red in only a couple of years.
Besides, new U.S. Department of Labor standards commanding
extra minutes pay for specialists not previously getting it
will help office costs, if and when they go live. In the home,
LTSS have been given by relatives, however later on, this
wellspring of care will be less accessible, in light of the
fact that relatives will work.
In spite of this mix of weights,
openings likewise exist. Keeping frail older people with chronic
diseases and inabilities out of intense care could spare a
considerable measure of cash, so "the open door at the
front end to truly take care of the Medicare cost issue is
a genuine one." Research additionally recommends that
home health services can play a significant cost-sparing part
in post-acute care also. To exploit such open doors, the home
medical services part will be required to record their cost
investment funds as well as the nature of the care that they
give. The blend of lower cost and excellent makes a strategic
offer for policy makers and citizens. Advance, the customary
division between healthcare services and LTSS needs to end.
The current problem is the fact that
policy makers are attempting to settle these programs at the
edges," when what is required is "a central reconsidering
of how we convey every one of these services."
Albeit innovative advances have settled
a substantial number of significant policy issues, it is not
clear what such progress would be. For instance, what organization
will affirm new health technologies devices? Are medical services
applications going to be regulated by the U.S. Food and Drug
Administration (FDA) or by the Federal Communications Commission?
At the point when an administration crosses state lines (as
with telehealth), challenges with state-based permitting and
extent of practice controls may emerge.
Trends in the Real
World
A few patterns help depict the truth
of U.S. home health care
" Restrictions in the Design
of the Medicare Home
" Health care Social Benefit
for Today's Population
A great many people are ignorant
of Home health care services until a snapshot of emergency,
when a staff member from the hospital, inpatient rehabilitation
center, or nursing home exhorts them that their cherished
one is being discharged and courses of action for care in
the home should be made. A great many Medicare recipients
who are older or have handicaps and their families have needed
to face this emergency and are accepting home services, however
the advantage is a poor fit to their requirements. Composed
right around 50 years prior, the Home health care advantage
underlines recuperation from intense sickness and the open
door for wellbeing change, and it presumes that the recipient's
issues will end. It doesn't underline wellness or prevention
, and it doesn't pay for solace care or palliation toward
the finish of life.
Patients getting Medicare Home health
care services must be home-bound, and once they are no longer
kept at home, the advantage closes. Be that as it may, "unending
malady goes on, [and] pharmaceuticals keep on coming into
the house,". By then, Home health care suppliers have
nobody to hand the patient over to or move to for ongoing
care and coordination. Understanding focused medical homes
take care of this issue, however they are a long way from
all inclusive.
Overseeing Continuous Transitions
In spite of these difficulties, Home
health care is being rehashed to fill in as a vital piece
in the continuum of perpetual care. In responsible care associations,
with their capitated structure, a few suppliers are working
around the strictures of the Medicare home medical services
advantage and ensuring that patients get the required administrations.
Moves not just between care settings-particularly healing
center to home-additionally amid the timeframe after a doctor's
visit are times when patients unquestionably require help,
even with an issue as essential as correspondence.
Despite these challenges, home health
care is being reinvented to serve as an important piece in
the continuum of chronic care. In accountable care organizations,
with their capitated structure, some providers are working
around the strictures of the Medicare home health care benefit
and ensuring that patients receive the needed services. Transitions
not only between care settings-especially hospital to home-but
also during the period of time after a physician's visit are
times when patients definitely need help, even with an issue
as basic as communication.
The home medical services nurse can sit with the patient and
relative or other parental figure and audit drugs, measurement
plans, and other therapeutic directions to help the family
get organized about the patient's health services needs. The
truth of wellbeing [care] in the house is the truth of the
kitchen table. That is the place wellbeing choices are made,
and that is the place wellbeing is overseen," The best
quality level of solution reconciliation occurs at the kitchen
table.
The most run of the mill issues,
are
o Remembering to take pharmaceuticals,
o Knowing what the symptoms of the
problems and when and from whom to look for assistance,
o Verifying that the individual or
family member(s) make an appointment with the community doctor
inside 1 to 2 weeks post-release and that the individual has
transportation,
o Making beyond any doubt that solid
plans for meal readiness are set up, and
o Checking the patient's capacity
to perform ADLs securely or whether courses of action are
expected to make these exercises less demanding or more secure
so that the individual can remain at home.
It is important to keep individuals
connected with every day?" Taking consideration of these
critical measurements of care will be essential to every patient
and family well past the 30 or 60 days of Medicare's home
medical services advantage or a post-acute care benefit.
Conclusion
There are a number of obstacles to synergistic work in home
medical services that should be overcome. For instance, doctors
assess pain differently from physical specialists, in contrast
so do the home wellbeing organization work force. Nor do these
three groups evaluate reliance in ADLs similarly, making it
more difficult to assess change or improvement. Besides, there
is a requirement for minimal basic common language for the
outcome measures.
Joint effort is an element of the
programs for dually qualified people, in which the objective
is better programmatic coordination all through the continuum
of care. This is to be accomplished through the integration
and arrangement of government Medicare and state Medicaid
reserves into a solitary source of monetary support for social
and additionally medical necessities.
Home health services does not imply
that a person is dependably in the home. It might mean having
a cell phone application that reminds a person to take medication;
it might be the accessibility of an attendant or pharmacist
through email or the phone. Responsive psychologically proper
and age-suitable correspondence frameworks would help stay
away from pointless police calls.
This work includes more than overseeing
ailment; it implies taking a wellness, preventive, and habilitation
approach. The idea of home health care is the fact that we
may not be able to offer full rehabilitation to the patient,
but we can help them live better in their home. This is what
we have to remember about the beauty of home care: it's at
home.
References
Beales, J. L., and T. Edes. 2009. Veteran's Affairs Home Based
Primary Care. Clinics in Geriatric Medicine 25(1):149-154.
CMS (Centers for Medicare & Medicaid
Services). 2012. Long-Term Care Minimum Data Set. http://www.cms.gov/Research-Statistics-Data-and-Systems/Files-for-Order/Identifiable
DataFiles/LongTermCareMinimumDataSetMDS.html (accessed January
22, 2015).
CMS. 2014. Jimmo v. Sebelius settlement
agreement: Fact sheet. http://www.cms.gov/Medicare/ Medicare-Fee-for-Service-Payment/SNFPPS/Downloads/Jimmo-FactSheet.pdf
(accessed December 30, 2014).
Coleman, E. A., C. Parry, S. Chalmers,
and S. J. Min. 2006. The care transitions intervention: Results
of a randomized controlled trial. Archives of Internal Medicine
166(17): 1822-1828.
Counsell, S. R., C. M. Callahan,
D. O. Clark, W. Tu, A. B. Buttar, T. E. Stump, and G. D.
Ricketts. 2007. Geriatric care management
for low-income seniors: A randomized con trolled trial. Journal
of the American Association 298(22):2623-2633.
De Jonge, K. E., N. Jamshed, D. Gilden,
J. Kubisiak, S. R. Broce, and G. Taler. 2014. Effects of home-based
primary care on Medicare costs in high-risk elders. Journal
of the American Geriatrics Society 62(10):1825-1831.
Demiris, N. A. 2011. A pragmatic
view on pragmatic trials. Dialogues in Clinical Neuroscience
13(2):217-224.
Edes, T., B. Kinosian, N. H. Vuckovic, L. O. Nichols, M. M.
Becker, and M. Hossain. 2014.
Better access, quality, and cost
for clinically complex veterans with home-based primary care.
Journal of the American Geriatrics Society 62(10):1954-1961.
Gage, B., M. Morley, P. Spain, and
M. Ingber. 2009. Examining post acute care relationships in
an integrated hospital system. Waltham, MA: RTI International.
Gage, B., M. Morley, L. Smith, M. J. Ingber, A. Deutsch, T.
Kline, J. Dever, J. Abbate, R.
Miller, B. Lyda-McDonald, C. Kelleher,
D. Garfinkel, J. Manning, C. M. Murtaugh, M. Stineman, and
T. Mallinson. 2012. Post-acute care payment reform demonstration:
Final report. Research Triangle Park, NC: RTI International.
IOM (Institute of Medicine). 2008.
Retooling for an aging America: Building the health care workforce.
Washington, DC: The National Academies Press.
Kaiser Family Foundation. 2014.Medicare
at a glance. http://kff.org/medicare/fact-sheet/
medicare-at-a-glance-fact-sheet (accessed December 31, 2014).
Leff, B., L. Burton, S. L. Mader,
B. Naughton, J. Burl, S. K. Inouye, W. B. Greenough III, S.
Guido, C. Langston, K. D. Frick, D. Steinwachs, and J. R.
Burton. 2005. Hospital at home: Feasibility and outcomes of
a program to provide hospital-level care at home for acutely
ill older patients. Annals of Internal Medicine 143(11):798-808.
MedPAC (Medicare Payment Advisory
Commission). 2013. Report to the Congress: Medicare payment
policy. Washington, DC: MedPAC.
Naylor, M. D., D. Brooten, R. Campbell,
B. S. Jacobsen, M. D. Mezey, M. V. Pauly, and J. S.
Schwartz. 1999. Comprehensive discharge planning and home
follow-up of hospital ized elders: A randomized clinical trial.
Journal of the American Association
281(7):613-620.
NRC (National Research Council).
2011. Health care comes home: The human factors. Wash- ington,
DC: The National Academies Press.
Rural Assistance Center. 2015. Promotora
de salud/lay health worker model. http://www. raconline.org/communityhealth/chw/module2/layhealth
(accessed January 23, 2015).
RWJF (Robert Wood Johnson Foundation).
2013. Cash & counseling. http://www.rwjf.org/en/ research-publications/find-rwjf-research/2013/06/cash---counseling.html
(accessed Janu- ary 23, 2015).
Shaughnessy, P. W., D. R. Hittle,
K. S. Crisler, M. C. Powell, A. A. Richard, A. M. Kramer,
R. E. Schlenker, J. F. Steiner, N. S. Donelan-McCall, J. M.
Beaudry, K. L. Mulvey-Lawlor, and K. Engle. 2002. Improving
patient outcomes of home health care: Findings from two demonstration
trials of outcome-based quality improvement. Journal of the
American Geriatrics Society 50(8):1354-1364.
Wieland, D., R. Boland, J. Baskins,
and B. Kinosian. 2010. Five-year survival in a program of
all-inclusive care for elderly compared with alternative institutional
and home- and community-based care. The Journals of Gerontology,
Series A: Biological Sciences and Sciences 65(7):721-726.
|

