| |
March
/ April 2017
- Volume 11, Issue 1
Physical abuse among Syrian refugee women in Jordan

|
 ( (
|
Noha Al-Shdayfat
Correspondence:
Noha Al-Shdayfat, PhD, RN
Princess Salma Faculty of Nursing,
Al al-Bayt University,
PO Box: 130040,
Mafraq 25113,
Jordan
Email: dr.nuhash@aabu.edu.jo; nohashdaifat@gmail.com
|
|
|
Abstract
Background: Physical abuse of women is the most
common form of female abuse all over the world.
Objective: The current study aimed to investigate
the prevalence of physical abuse and its association
with some socio-demographic variables among Syrian refugee
women in Jordan.
Methods: 182 Syrian refugee women visited the
Maternal and Child Health Centers (MCHC) in Mafraq district
and participated in the current study during March 1,
2014 and June 1, 2014. The Arabic version of the NorVold
Domestic Abuse Questionnaire (NORAQ) was used to collect
data from the study participants.
Results: The study findings revealed that about
one third of the participants (57, 31.3%) experienced
physical abuse (before and after refuge). Twenty seven
participants (14.8%) reported being physically abused
during the last year. Husbands were the perpetrators
in 38.6% of the physical abuse acts reported by the
participants, followed by fathers (14%) and brothers
(10%). The bivariate analysis revealed that educated
women, older women, those who come from small size families
(<6 members), and those who got married at or after
21 years of age were less likely to report physical
abuse. The regression model analysis showed that educational
level of the physically abused women is the strongest
contributing factor to predict their psychological suffering
scale (Beta= -1.7, p < 0.05) followed by marital
status and household income (Beta= -1.3, and 0.94 p
< 0.05) respectively.
Conclusion: The current
study will pave the way to fill the gap in the literature
in regard to physical abuse prevalence and the associated
factors among Syrian refugee women in Jordan. However,
further research will be needed to address this important
issue.
Key words: Physical abuse, Refugee, Syrian women,
Jordan
|
Background
Physical abuse against women is defined by the United Nations
as "any act of gender-based violence that results in,
or is likely to result in, physical, sexual or mental harm
or suffering to women, including threats of such acts, coercion
or arbitrary deprivation of liberty, whether occurring in
public or in private life."
Domestic violence is a worldwide public health concern. However,
high vulnerability of women in developing countries increases
the risk of being battered by husbands and / or a family member
(1). Social and cultural norms in the Arabic societies allow
men to discipline women by physical acts such as beating (2).
In such patriarchal societies, the political and legal context
may contribute to the increase in violence against women (3).
Also, legislation and traditional practices do not criminalize
violence against women, but justify it through religion, culture,
and often the health authorities and security or legal authorities,
consider violence against women as a family interest and must
not be shared with the outsiders. Domestic violence prevalence
against immigrant or refugee women in the host countries might
not exceed the rates in the original countries. However, the
vulnerability for refugee women is expected to escalate, because
they lost their resources such as their families and support
systems (4).
Violence against women in Arab world
has not been sufficiently studied (5). High prevalence of
physical abuse against women has been reported by few studies
conducted in the Mediterranean and North Africa region. One
of such studies that collected data on physical violence from
262 women living in Palestinian refugee camps in Jordan found
that 44.7% of the women participants reported lifetime beating
(3). Similarly, the findings of a study conducted in Saudi
Arabia showed that 25.7% of the women in Medina district reported
being physically abused by their husbands (6).
Some research suggested an association between poor socio-demographic
conditions and physical abuse and wife beating. For example,
the results of a survey carried out in 2005 on the prevalence
of wife beating in Egypt revealed that women who live in urban
areas were less likely to be beaten by husband than that of
those who live in rural areas, and women whose first marriage
was at 30 years old and more were at higher risk for wife
beating (7). Women's age and educational level were also found
to have an inverse association with physical violence against
women (8, 9). Other research linked household income with
physical wife abuse (10, 8)
In previous research physical abuse has been reported to coexist
with emotional abuse (11, 5, 12, 2, and 13). In addition women
who are physically abused by their husbands were often abused
by another person such as a family member (11).
Reporting physical abuse to a health
professional and/or talking about it to a friend or a family
member is the first step to break the cycle of the domestic
violence. Yet, many women hesitate to discuss their status
with anyone because they fear to lose their husbands, housing
and/or children (Gender-Based Violence Area of Responsibility
(GBV AoR), DRAFT - Guidelines for Integrating Gender-Based
Violence Interventions in Humanitarian Action, 2014) especially
if they are financially dependent on them. Other reason might
be the socio-cultural norms in the Arab conservative societies
that stigmatize the divorced or separated woman as a bad person.
Thus, low reporting of physical abuse is expected, particularly,
among the disadvantaged communities such as refugees and immigrants
in developing countries where only 7% of gender based violence
is officially reported cases.
Psychological consequences of women abuse might be similar
or even more serious than that of physical consequences; depression
is one of the most frequently reported psychological consequences
of the physical abuse against women (14, 15).
Being the first to investigate physical
violence against Syrian refugee women in Jordan, this study
aimed to investigate lifelong prevalence and current prevalence
(last year) of physical abuse. In addition, the study aimed
to explore the association of some socio-demographic factors
with the occurrence of physical abuse among Syrian refugee
women in Jordan.
Methods
Ethical Approval
A descriptive cross-sectional design was used to investigate
the prevalence of physical abuse among Syrian refugee women
in Jordan. Ethical approval has been gained from the IRB committee
in Al al-Bayt University and the Jordanian Ministry of Health.
Also, consent to participate in the study was obtained from
the women who were invited into the current study.
Population
Participants were recruited from Maternal and Child Health
Clinics (MCHCs) in Mafraq governorate. All Syrian women who
are able to read and write Arabic language, aged 18 or older,
and visited the MCHCs during the period (March 1, 2014 and
June 1, 2014) were invited to participate in the study. From
the 280 women who were invited to participate, 205 women agreed
to participate in the study with a response rate of 73%. However,
23 partially filled questionnaires were excluded from analysis.
Accordingly, a convenient sample of 182 women was obtained.
Instrument
The validated Arabic version of the NorVold Domestic Abuse
Questionnaire (NORAQ) was applied to measure the physical
abuse. Permission to apply the instrument was gained from
Linda Haddad who translated and validated the tool (11).
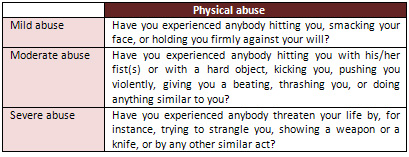
The NORAQ questionnaire includes
five parts (emotional abuse, physical abuse, and sexual
abuse, current experience of abuse, and experience of reporting
abuse to primary care personnel.
Table 1: Detailed questions of
physical abusive acts
The last section of the questionnaire included questions on
socio-demographic characteristics of the participants, such
as age, level of education, marital status, place of residence,
family size, household income, marriage age, and working status.
Age was categorized into 25 years or less, and 26 years and
above. Level of education was also measured by a binary variable:
primary education, and secondary or more. Household income
distinguished women who live in a household with monthly income
of 200 JD or less, and more than 200JD. Place of residence
refers to rural and urban.
Procedure
Research assistants where trained to collect the data from
the participants. They approached the women in the MCHCs.
The questionnaires were distributed and explained to the participants.
To ensure confidentiality participants who agreed to participate
in the study were asked not to write their names or addresses.
Statistical
Analysis
Statistical analysis was performed using SPSS for Windows
19. Descriptive statistics including frequencies were used
to describe participants' characteristics. Chi square tests
were used to describe association between women's exposure
to physical abuse and some socio-demographic variables. Independent
samples t test was used to assess for differences in psychological
suffering scores between abused women from different socio-demographic
groups. Linear regression models were applied to predict the
contributing variables to physical abuse. A significance level
of .05 was the cutoff point.
Results
Socio-demographic characteristics of the participants
Participants' ages ranged from 19 to 55. Sixty seven women
(36.8 %) live in the rural areas and 115 women (63.2%) of
them live in the city of Mafraq. Most of the participants
(73.1%, N=133) had finished their primary education, and about
one fifth (23.1%, N=42) of the participants had graduated
from high schools, and only five participants (2.7 %) and
two participants (1.1%) had graduated from a college and a
university respectively. Most of the sample were married women
(78.6%, N= 143) while the rest of the participants were single
(9.9%, N=18), widowed (8.2%, N=15), and divorced (3.3%, N=6).
Most of the participants' household income was 200 JD or less
(88.5%, N=116).
Prevalence of physical abuse by socio-demographic characteristics
of the participants
About one third of the participants (57, 31.3%) reported a
lifetime experience of physical abuse (before and after refuge).
Of these, more than one quarter (25.3%, 46 participants) reported
mild physical abuse. Some 44 participants (24.2%) experienced
moderate physical abuse. About 14 participants (7.7%) experienced
severe physical abuse. The sum of the participants experienced
the three types of physical abuse is more than 57 because
many of them reported being exposed to more than one type
of physical abuse (mild, moderate, and severe) (Table 1).
Twenty seven respondents (14.8%,
27) were exposed to physical abuse during the last year. Twenty
two married participants (38.6%) reported that their husbands
were responsible for the abuse that they were exposed to,
followed by fathers (14%, 8 participants), and brothers (10%,
6 participants). About one quarter of the participants (23%,
43 participants) reported being physically and emotionally
abused.
The bivariate analysis revealed that
some socio-demographic characteristics are significantly associated
with exposure to physical abuse among the Syrian refugee women.
For example, educated women were less likely to report exposure
to physical abuse than those who are less educated (x²=4.43,
N = 182, p =0.035). Also, participants who live in households
with large family size (6 members and more) were more likely
to report being physically abused (x²=4.16, N
= 182 p =0.041). Older participants (older than 25 years old)
reported being exposed to physical abuse more than those who
were aged 25 years or less (x²=4.57, N = 182 p
=0.032). In addition, women who were married before their
20th birthday reported being physically abused more than those
who were married in older age (x²=3.96, N = 155)
p =0.047). However, other demographic groups within the study
sample were not significantly associated with physical abuse
(i.e. marital status, place of living, and household income).
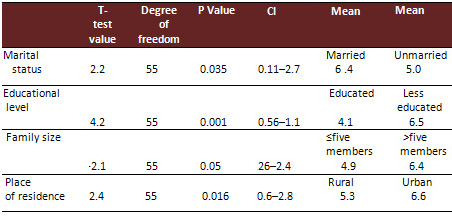
Higher psychological suffering was
reported by the participants who are married, less educated,
living in large family size households, and living in urban
area (see Table 3). Other factors such as household income,
husbands' employment status, participants' age and marriage
age showed no significance difference in terms of psychological
suffering score.
Regression analysis findings showed that some socio-demographic
variables of the participants were contributed to the variance
in psychological suffering score (as reported by physically
abused women). A significant regression model was found (the
enter method was performed), F = 6.1, p = 0.00. The revealed
model explains 31.5 percent of the variance in the participants'
suffering score. The correlation matrix between the independent
variables showed no evidence of multicolinearity. Educational
level was the strongest contributor to the variance in the
suffering score (Beta= -1.7) followed by marital status and
household income with Beta values -1.3 and, 0.94. The regression
analysis results shows that women who were educated, not married
and have higher household income were less likely to report
high scores in the psychological suffering scale.
Table 2: The associations between
the psychological suffering and the participants' marital
status, educational level, family size, and place of residence
(N = 57)
The association of physical
abuse with some mental health disorders was investigated.
The findings showed that physical abuse is significantly associated
with experiencing depression (x²=4.51, N = 182,
p =0.034). On other hand, anguish feeling and insomnia were
not found to be significantly associated with experiencing
physical abuse among the study sample.
Discussion
The current study produced several interesting findings. First
of all, though lifetime prevalence of physical abuse against
refugee Syrian women was high (31.3 %) (i e it is higher than
that in Saudi Arabia (25.7%)) (6). Yet, it seems relatively
low compared to the findings of other investigations conducted
in the region and other parts of the world. The prevalence
rate of lifetime physical abuse of some regional studies'
findings is higher, for example, 44.7% among Palestinian refugee
women living in Palestinian refugee camps in Jordan reported
lifetime physical abuse (3). The reason behind this might
be that the Palestinian women in this study were recruited
from the refugee camps while Syrian refugee women in the current
study are non-camp dwellers. There is no doubt that comparing
the current prevalence rates of physical abuse with that of
previous research in the regional, refugees and immigrant
populations is beneficial. Though, it is worth noting the
timeframe and methodological variations among different studies.
Disadvantaged socioeconomic circumstances,
in which the refugee women live, put them at higher risk of
being victims of abuse. Similar to other studies, the results
of the current study showed a significant association between
low educational level and the likelihood to be a victim of
physical abuse (8, 9) In contrast, the current study findings
were incongruent with those of the previous research (8, 10)
where the household income was not found to be associated
with physical abuse. The current study revealed that less
educated women and those who live in households with large
family size and women who got married before their 20th birthday
are more vulnerable to physical abuse. In addition, almost
all women who participated in the study are housewives, thus
they are financially dependent on their husbands or male family
members.
The present study provides further evidence that physical
abuse often coexists with emotional abuse among women. The
current study findings are congruent with the previous studies
(11, 5, 12, 2, 13); 23% of the participants reported that
they were physically abused alongside the emotional abuse
A closer look at the current research findings showed that
few participants had reported the exposure to physical abuse
(one of the most under-reporting types of domestic abuse in
the developing world). Only 6% of the Syrian refugee women
who participated in the study reported the physical abuse
to health care providers.
Limitations
The main limitation of the current study is that it employed
a non-probability sampling technique (a convenient sample)
which may affect the generizability of the findings. Also,
the study participants were non-camp refugees. Thus, further
research will be needed to understand the physical abuse phenomena
among Syrian refugee women who live in devastating living
circumstances in the refugee camps.
Recommendations
This is the first study to report physical violence and its
associated factors among Syrian refugee women in a country
that hosts refugees. Mental health services are needed and
nurses and physicians should be trained to provide proper
counseling for these women, particularly because we found
a significant association between exposure to physical abuse
and poor emotional health suggests a need to integrate mental
health and GBV.
Finally, given that we report a relatively high prevalence
of physical abuse yet we know current GBV programming for
the non-camp population to be inadequate, we suggest an immediate
scale-up of GBV interventions to prevent GBV and mitigate
its consequences among Syrian refugee women in non-camp settings.
References
1. WHO. World report on violence and health. (2002).. In:
Krug EG, Dahlberg LL, Mercy JA, et al, eds. Geneva: World
Health Organisation
2. AL-Badayneh, D. (2004). The national scope for protection
of Jordanian families from family violence. Amman, Jordan:
National Council for Family Affairs
3. Khawaja M, Barazi R. (2005). Prevalence of wife beating
in Jordanian refugee camps: reports by men and women, J Epidemiol
Community Health 59:840-841. doi: 10.1136/jech.2004.031625
4. Menjivar C. and Salcido O. , (2014) . Immigrant Women and
Domestic Violence
Common Experiences in Different Countries. Gender society.
Sage publications.
5. Btoush, R., & Haj-Yahia, M. M. (2008). Attitudes of
Jordanian society about wife abuse. Journal of Interpersonal
Violence, 23(11), 1531-1554
6. Tashkandi A, Rasheed FP. Wife abuse: a hidden problem.
A study among Saudi women attending PHC centres. East Mediterr
Health J 2009;15:1242-53 [PubMed]
7. Akmatov MK , Mikolajczyk RT , Labeeb Sh , Dhaher E , and
Mobarak Khan Md (2008). Factors associated with wife beating
in Egypt: Analysis of two surveys (1995 and 2005). BMC Womens
Health; 8(15).
8. Koenig, M. A., et al. (2003). Domestic violence in rural
Uganda: evidence from a community-based study. Bulletin WHO,
81,53-60
9. Ahmad Kh, Sheikh KS, Chatha SA. (2014). Socio-economic
Status and Domestic Violence: A Study on Married Women in
Urban Lahore. A Research Journal of South Asian Studies; 29(1),
pp. 229-237
10. Jejeebhoy SJ and Cook RJ (1997). State accountability
for wife-beating: the Indian challenge. Lancet 349 Supplement
l: SI10-2.
11. Haddad LG, Shotar A, Younger JB, Alzyoud S, Bouhaidar
CM. (2011). Screening for domestic violence in Jordan: validation
of an Arabic version of a domestic violence against women
questionnaire. International Journal of Womens' Health, 3,
79-86.
12. Garcia-Moreno, C., Jansen, H., Ellsberg, M., Heise, L.,
& Watts, C. (2006). Prevalence of intimate partner violence:
Findings from the WHO multi-country study on women's health
and domestic violence. Lancet, 368 , 1260-1269.
13. Coker AL, Davis KE, Arias I, Desai S, Sanderson M, Brandt
HM, Smith PH. Physical and mental health effects of intimate
partner violence for men and women. 2002; Am J Prev Med.;
23(4):260-8.
14. Campble J C 2002. Health consequences of intimate partner
violence) Lancet; 349 (9314) p 1333-1336
15. Devries KM, Mak JY, Bacchus LJ, Child JC, Falder G, Petzold
M, Astbury J, Watts CH. (2013). Intimate partner violence
and incident depressive symptoms and suicide attempts: a systematic
review of longitudinal studies. PLoS Med 2013; 10: e1001439.
|
 |

