| |
April
2013 - Volume 7, Issue 2
Producing and
utilising research: Barriers for a nursing faculty in Oman

|

(
|
Gillian White
Correspondence:
:Professor Gillian White
SCM., RM., MTD., Cert Ad Ed
BEd., Dip.Soc.Sci (Psych), MA (Hons), PhD
Education Advisor
Directorate General Education and Training
Ministry of Health
Sultanate of Oman
Email:
drgillianwhite@yahoo.co.nz
|
|
|
Abstract
Background and Objectives: One year specialised
nursing programmes for registered nurses are undertaken
in one national institute in Oman, however there is
very little nursing research conducted or published
by the faculty. The study was conducted to discover
the barriers to the production and utilization of research
from the perspective of the faculty at the specialized
nursing institute in Oman.
Methods: The BARRIERS scale has been used extensively
to identify barriers to research utilization. This scale
was chosen and adapted to identify barriers to research
production as well as utilisation in this specialised
institute. The survey tool was divided into two main
sections, the production of research and the utilization
of research. All available faculty members were invited
to take part and sixty two percent participated.
Results: Accessibility, facilities and aspects of
the research itself were seen as barriers to the utilization
of research, while time, workload and lack of motivation
were perceived as barriers to producing research.
Conclusion: In order to produce clinical nurses
who deliver evidence based specialised nursing practice,
the facilities and support for research by the faculty
must be prioritized in the education setting.
Key Words: Nursing, Nursing Education and Research,
Evidence based practice
|
Introduction
One objective of the Oman Ministry of Health (MoH) 8th Strategic
Plan 2011 - 2015 (1) is "to enhance the capabilities
and skills of teaching staff and students on approach and
methodology of scientific research" (p.4). The MoH estimated
that in 2010 only 2 percent of the faculty who had been trained
in research design and methodology had conducted research.
There are no estimates of "research utilized for planning
and improving teaching and related activities" (1).
The MoH one year post-basic specialized nursing Diploma programmes
for registered nurses emphasizes evidence based practice and
includes a core research paper. Only the specialized Community
Health programme is at Bachelor degree level and that contains
a module on Evidence Based Practice taught by faculty from
Cardiff University.
In this paper the production and utilization of research by
faculty at the only specialized nursing institute in Oman
is explored using the BARRIERS to research utilisation questionnaire
(2, 3, 4).
Literature
The gap between research findings and the utilization of research
by nurses has been discussed over many decades (5). A systematic
review of sixty three studies identified that barriers appeared
consistent over time and across geographic locations (6).
Barriers to utilizing research in clinical practice are complex
with several overlapping factors (7). Reports list time constraints,
lack of awareness of available literature, insufficient authority
to make changes, inadequate skills in research appraisal and
lack of support to implement change based on research evidence
(8). One descriptive study, from the Arab world, to identify
barriers and facilitators of research utilization among Iranian
nurses (9) demonstrated consistency with Western findings
such as time, inadequate facilities, and lack of authority.
An overview of current literature about barriers to research
utilisation from scientific nursing journals, focusing on
two hundred and twenty six articles published between 1995
and 2005, found that barriers related to the organisation,
communication of research and the nurses' competence in clinical
research, strongly suggested education institutes needed to
increase nurses' research knowledge and skills, and provide
nurse educators with research time (7).
As there were no studies found exploring barriers to producing
research and therefore no suitable tool available, the BARRIERS
tool was modified to apply to nursing educators.
The BARRIERS tool
The survey tool on barriers to research utilization in clinical
practice used in the reported research is the validated Barriers'
Scale (2, 3, 4). The authors (2) believed that a barrier hindering
the implementation of change was the lack of an effective
diagnostic tool. After studying the literature the team developed
the BARRIERS scale based upon Rogers' theory of diffusion
of innovation (10, 11). Change is perceived to depend on the
Characteristics of the Adopter; the Characteristics of the
Organization; the Characteristics of the Innovation; and the
Characteristics of the Communication. They also studied the
Code and Utilisation of Research in Nursing (CURN) project
where nurses were supported to implement the findings in practice
(12). The validity and reliability of the BARRIERS scale were
tested along with an investigation of the relationship between
the four factors in Rogers' model (2).
A review of forty five studies where the BARRIERS scale had
been used found the same barriers predominated (13). With
continuous consistency over the years it raises questions
about why the barriers have not been overcome (6).
While an assumption was made that similar findings would be
found among the specialty nursing faculty in Oman the research
was specifically conducted with the aim of making transparent
the perceived barriers to management so that rationale for
implementation of change was supported by evidence. An advantage
with the current study is the MoH objective to enhance the
capabilities and skills of the teaching staff in research.
Unlike countries where similar studies were conducted, utilization
(and production) of research is supported by the Oman government
which makes strategies for change more likely to be implemented.
Aim
The aim of part one was to identify barriers to the utilisation
of research. The aim of part two was to identify barriers
to the production of research as perceived by the faculty
of the nursing specialty institute.
Design
A modified BARRIERS survey was divided into two main sections:
the utilisation of research using the full BARRIERS to research
utilization survey; and a modified version on research production,
adapted to reflect nursing education through minor changes
where the words "nursing education' replaced "clinical
practice".
Part one consisted of thirty questions and Part two consisted
of sixteen questions where respondents were asked to rate
each item on a 4 point Likert scale from 1 = no affect to
4 = a great deal of affect plus a fifth 'no opinion' option.
Open ended questions were included for the respondents to
add barriers.
In this study the characteristic divisions Adopter, Organization,
Innovation, and Communication (2) were identified as the Nurse
[in this case Faculty], the Setting, the Research, and the
Presentation and Accessibility of the research as previously
modified (5).
Ethics approval
The proposal was approved by the Institute Research Committee
and permission was obtained from the Dean. Faculty was informed
by memorandum about the aims, purpose and details. Each questionnaire
was numbered and the number matched to a master list held
by the Dean's office where only one administrator (non researcher)
had access to the list (but not the questionnaires). Non-responders
were reminded on two occasions by the administrator. The researcher
was not aware of who had responded. At the end of the data
collection period the master list was shredded by the administrator
to ensure that anonymity and confidentiality were maintained.
Consent was implied by return of completed questionnaire.
The statistics for the institute indicated a male to female
ratio of 1:3 and a mean age of 45 years. One faculty member
held a PhD, twenty four held Master's degrees, and twelve
Bachelor's degrees. All available faculty were invited N =
37 and n= 23 (62%) faculty responded. Some members were on
long term leave or absent for various reasons. The number
was considered representative of the total faculty. Feedback
to the faculty and their response about the results confirmed
the overall interpretation and findings.
Analysis
As the group of respondents in the current study was small
the analysis was confined to the descriptive level. Frequencies
of responses to each question were tabled on an Excel sheet.
The mode of response per question was colour-coded to represent
"little barrier," "moderate barrier" and
"a great barrier." The results are outlined as Part
One (Barriers to research utilization) and Part Two (Barriers
to production of research).
Results (Part ONE):
Utilisation
Questions 1, 6, 12, 13, 19 clustered at Likert 4 "a great
barrier" and Questions 7, 24, 26 clustered at Likert
3 "a moderate barrier "as shown in Table 1.
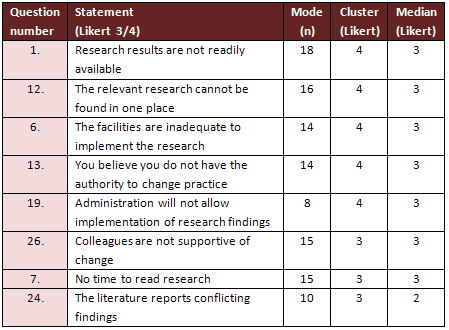
Table 1: Factors perceived as moderate to great Barriers
Two of the great barriers (Statements 1, 12) concern the Characteristics
of Presentation and Accessibility of research. Five statements
(6, 7, 13, 19, 26) concern the Setting; and one (24) the Research
itself.
Qualitative responses
From the qualitative responses, the greatest barrier concerned
lack of support (both collegial and by authorities) to be
able to make changes.
"Other colleagues are not supportive of change"
"Resistance to change by clinical people"
Other comments suggested that there was "lack of statistical
abilities to be able to understand quantitative research";
"resistance to change"; "inadequate facilities";
"poor participation in research because of lack of knowledge
and practice of how to do it right." Staff felt "isolated
from colleagues who are interested in research". Some
did "not see the value of doing research in their current
position."
RESULTS (Part TWO):
Production
As very little research was being produced the differentiation
between the two categories "moderate and great"
was not meaningful. Therefore the moderate and great barrier
results were collapsed into one domain and percentages were
calculated. The main barriers to producing research are shown
in Table 2 along with a description. In addition, while 63.6%
considered their managers were very supportive of research,
77.3% had no interest in personal benefits of producing research.
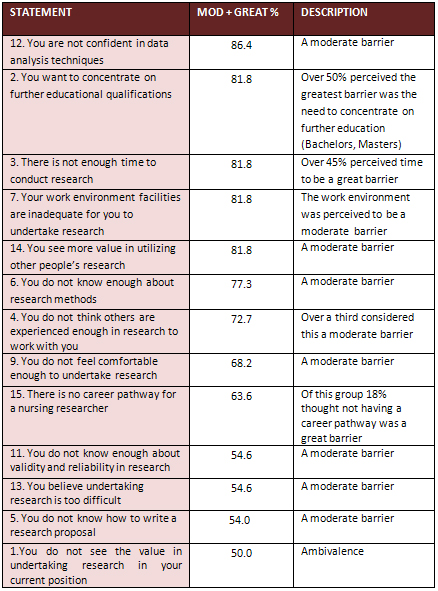
Table 2: Factors perceived as Barriers to the Production
of Research
Qualitative responses
Free responses highlighted the need for confidence, a healthy
environment and fairness in workloads. Assistance from an
experienced research committee and statistician plus access
to databases, were also seen as important facilitators of
being able to produce research.
The three greatest barriers described were:
i) Time - "there is not enough time to conduct
research"
ii) Workload - "negative attitude of people toward
research means there is no reduction in workload"
iii) Lack of drive and passion to undertake research
- "it takes effort" "there is no initiative."
Discussion
The analysis of Likert scales has been debated with some arguing
the data should be treated as ordinal and others as interval
(14). In this study the group is homogenous which delimits
the variability and the data is considered ordinal in that
there is a logical ordering of the categories. Some statisticians
recommend using the median and mode for such data (15) as
order is relative and shows only sequence. Thus the decision
was made to report the median and mode of response to each
question in part one and the percentages in part two.
In part one three factors were identified -
1) the Research,
2) the Setting, and
3) the Presentation and Accessibility of the research. Five
organizational concerns relating to Setting can be summarized
as Barriers regarding facilities, time, authority, implementation
and collegial support. While other factors regarding the ability
to find relevant research and manage conflicting research
results present as Faculty and Presentation/Accessibility
of research characteristics, they may also be viewed as strongly
linked to the Organisation/Setting.
In one of the responses (item 24: "The literature reports
conflicting findings") the median is different to the
median of the other responses indicating the barrier is actually
small to moderate. In item 19 "Administration will not
allow implementation of research findings" the mode is
small although the median demonstrates a moderate barrier.
This latter result is skewed by the larger number of "no
opinions" recorded (7).
An Australian study (8) surveyed 761 nurses' opinions regarding
the barriers and the facilitators of research utilization.
The barriers were time constraints, lack of awareness of available
literature, lack of authority to change practice, inadequate
research skills in particular critique and lack of support
for implementation of change. The faculty in this study, as
seen in Table 1, had similar opinions albeit in the education
setting. Such findings are "remarkably consistent with
studies in the USA, UK and Northern Ireland" (8, p.304).
In part two (production of research) four of the barriers
are related to the characteristics of the Setting: time, other
experienced staff to work with, inadequate facilities and
lack of career path for researchers. Faculty characteristics
however were also visible and cluster around lack of knowledge
and experience in research. The drive to gain Bachelor's,
Master's or PhD qualifications is paramount to be eligible
for better positions. Thus the ambivalence about the value
of producing research in the current position may reflect
an organizational priority to produce teachers, not researchers.
Indeed, the lack of concern about personal benefits gained
from producing research emphasizes the compulsion to gain
higher academic qualifications. While management was supportive
and many of the factors are under managerial control, the
focus was on acquiring suitably qualified specialist nursing
teachers and research outputs were not rewarded.
Little nursing research has been undertaken in Oman as research
utilization and evidence based nursing practice is a fairly
new concept and nursing research in its very early stages
of development. However a study to identify barriers and facilitators
to research utilization was undertaken in Iran among 410 nurses
from educational hospitals and nursing schools associated
with Tehran Medical Sciences University (9). The findings
are similar to those found in this Oman study: time, inadequate
facilities, not enough authority to change practice. The authors
categorized the findings into two main groups i.e. organization
and human resources. They concluded that the Iranian health
care system did not provide incentives for nurses to engage
in or read research due to time availability through nurse
shortages and stated that "the most important organizational
change that needs to occur is the provision of available facilities
for nurses to use research evidence" (9, p. 2194).
Some authors (6, 13) have argued that identifying barriers
has not provided evidence of change. Rather nurses outside
of North America were significantly more likely to view inadequate
facilities as a barrier (6). It is important that the organization
in this study supports research by providing the required
research environment and adjusting workloads so that faculty
can prepare and support specialty nurse graduates utilize
research and implement change on return to clinical practice.
In part two of the study, ten of the statement responses are
Faculty and four are Setting (a ratio of 5:2). Most barriers
to producing research are related to issues such as abilities,
motivation and confidence. The concept of time as a barrier,
however, may not signify 'real time' but rather indicate improper
use of time due to lack of motivation through lack of energy,
knowledge and reward. In a Norwegian study (16) heavy workloads
resulted in nurses being too tired to undertake research related
activities.
The opportunity to read, plan, implement, analyse and write
up research reports as a legitimate activity during working
hours must be provided by the organization if the strategic
research goals are to be met. In addition, while there is
an admirable drive to increase the number of PhD nurses in
Oman, and full scholarships are being awarded, most of the
candidates are prepared for research only in theory.
Conclusion
The Nursing Institute should not be singled out as failing
to provide an environment conducive to research as the findings
demonstrate that the same barriers exist throughout much of
the nursing world. However, the findings should alert the
authorities that, in order to produce clinical nurses who
deliver evidence based practice, the facilities and support
for research must be prioritized in the nursing educational
settings, where the nurse educators can act as role models
for research. This prioritization is especially important
when the vision is to upgrade entry to the nursing profession
to baccalaureate level and nursing specialization programmes
will transit from diploma to baccalaureate and master's degrees.
Research is now needed to explore whether there is a relationship
between perceptions of barriers to research utilization and
production, and the utilization of evidence based practice
in the education and practice of nurses contextualized to
the Omani culture and health service environment. Engaging
nurses in research in Oman is most important and opportunities
to practice hands on research can only add to the success
of their future studies.
Acknowledgements: the Ministry of Health, Oman, for
the time and financial support.
Ms Muna Ramadan for organizational assistance.
References
1. Author. Ministry of Health Strategic plan 2011
- 2015. 2011 (English version). Oman: MoH.
2. Funk SG, Champagne MT, Wiese RA, Tornquist EM. BARRIERS:
The barriers to research utilization scale. Applied Nursing
Research 1991a; 41: 39 - 45.
3. Funk SG, Champagne MT, Wiese RA, Tornquist EM. Barriers
to using research findings in practice: the clinician's perspective.
Applied Nursing Research 1991b; 4(2): 90-95.
4. Funk SG, Tornquist EM, Champagne MT. Barriers and facilitators
of research utilization. Nursing Clinics of North America
1995; 30: 395 - 407.
5. Bryar R, Jose Closs S, Baum G, Cooke J, Griffiths J, Hostick
T, Kelly S, Knight S, Marshall K, Thompson DR. The Yorkshire
BARRIERS project: diagnostic analysis of barriers to research
utilization. International Journal of Nursing Studies 2003;
40(1): 73 - 84.
6. Kajermo KN, Bostrom A-M, Thompson DS, Hutchinson AM, Estabrooks
CA, Wallin L. The BARRIERS scale - the barriers to research
utilisation scale: A systematic review. Implement Sci 2010;
5:32. Published online 2010 April 26. doi: 10.1186/1748-5908-5-32
7. Markussen K, Forskningssykepleier F. Barriers to research
utilization in clinical practice. Vard I Norden Nordic Journal
of Nursing Research and Clinical Studies 2007; 83(27):
47 - 49.
8. Hutchinson AM, Johnston L. Bridging the divide: a survey
of nurses' opinions regarding barriers to and facilitators
of, research utilization in the practice setting. Journal
of Clinical Nursing 2004; 13: 304 - 315.
9. Mehrdad N, Salsali M, Kazemnejad A. The spectrum of barriers
to and facilitators of research in Iranian nursing. Journal
of Clinical Nursing 2008; 17: 2194 - 2202.
10. Rogers EM. Diffusion of Innovations (1st edn.). New York:
Free Press, 1983.
11. Rogers EM. Diffusion of Innovations (5th edn.). New York:
Free Press, 2003.
12. Horsley JA, Crane J, Crabtree MK. Using research to improve
nursing practice: a guide CURN project. New York: Grune and
Stratton, 1983.
13. Carlson CL, Plonczynski DJ. Has the BARRIERS scale changed
nursing practice? An integrative review. Journal of Advanced
Nursing 2008; 63(4): 322 - 333.
14. Miles J, Shevlin M. Applying regression and correlation:
A guide for students and researchers. London: Sage Publications,
2001.
15. http://www.childrensmercy.org/stats/definitions/ordinal.htm
retrieved 18 July, 2011.
16. Hommelstad J, Ruland CM. Norwegian nurses' perceived barriers
and facilitators to research use. Aorn Journal 2004; 79: 621-634.
|
 |

