| |
April
2013 - Volume 7, Issue 2
Determinants
of Current Contraception Use among the Ever- married Females
in Rajshahi District of Bangladesh

|

(
|
Jahirul Islam
(1)
Shahin Reza (2)
(1)
Md. Jahirul Islam
Ministry of Health and Family Welfare, Bangladesh Secretariat,
Dhaka-1000, Bangladesh.
(2)Md. Shahin Reza
Department of Population Science and Human Resource
Development,
University of Rajshahi, Rajshahi-6205, Bangladesh.
Correspondence:
Md. Jahirul Islam
Assistant Chief (Family Welfare-3 Section)
Ministry of Health and Family Welfare
Bangladesh Secretariat, Dhaka-1000, Bangladesh
Email:
mdjahirul@yahoo.com
|
|
|
Abstract
The aim of this paper is to investigate the determinants
of current contraception use of the ever-married females.
Using the information from 2000 ever married women of
Rajshahi district, within the reproductive span (15-49
years), we found that among the factors determining
contraceptive use among women, education appears to
be the most significant; education is positively associated
with contraceptive use. The region of residence, occupation
of husband and bank account ownership, visits of family
planning workers and talking to husbands about family
planning also appear to be significant factors determining
the level of contraceptive use among the women. Again,
we found that, number of living children to a woman
is also associated with the use of contraception. The
result shows that women who have no living children
are less likely to use any method. This study also envisages
that, most women, both in rural and urban areas use
modern methods more frequently than traditional methods.
This study intends to examine the current use of contraception
and helps in understanding the influences of various
socio-demographic factors in raising the current use
of contraception in Rajshahi district.
Key words and Phrases: Contraception, Fertility
preference, Rajshahi District, Logistic regression analysis
|
Introduction
Any deliberate practice to reduce
the risk of conception is considered as contraception. Contraceptive
use is the most frequent proximate determinant of age at first
birth and fertility. Contraception can delay the first birth
and reduce fertility by either spacing or limiting births.
Therefore, it is necessary to understand the levels and determinants
of contraceptive use in order to formulate policies supporting
proper strategies for raising contraceptive prevalence.
Contraceptive use is one of the crucial
factors mediating between sexual activities and conception
and it is one of the oldest methods of fertility reduction.
The use of contraceptives is the most important factor that
directly affects fertility. Rising use of contraception is
undoubtedly the main proximate determinants of the ongoing
fertility decline in developing countries like Bangladesh
(Bongaarts,J 1991). Since independence, contraceptive prevalence
has steadily grown in Bangladesh. Contraceptive Surveys conducted
at the national level indicate a rising trend in the contraceptive
prevalence rate.
Between 1975 and 1999-2000, current use of contraceptive methods
has increased from 7.7% in 1975 to 53.8% in 1999-2000 (BDHS,
1999-2000).
Several authors have argued that
Bangladeshi couples are not likely to adopt contraception
until they experience improvements in their socio-economic
condition (Khuda, B.J. Stoeckel and N. Piet-Pelon, 1997).
Social and economic development as well as more widely diffused
family planning services will contribute to a higher level
of contraceptive use. Various studies indicate that current
use of contraceptives and acceptance of small family norm
depends on a number of factors like education, place of residence,
occupation and so on (Coutris, S.; Ullah and Chakraborty,
1993). Ross and E. Frankenbreg (1993) observed that effort
of family planning programs and socioeconomic conditions exert
both independent and joint effects on family size. For instance,
educational attainment of the woman is generally considered
to be a useful index of socioeconomic status as well as of
the level of overall social sophistication and therefore,
it is inversely related to the desire for additional children
and positively related to the use of contraception. Similarly,
mobility of women outside the home creates opportunity to
the improvement of women and increases the social status of
poor women and consequently their attitude towards family
planning as well as contraceptive use (Duza and M.Nag, 1993).
In addition, high infant and child mortality is also an important
determinant of contraceptive use in Bangladesh. At least one
out of ten children dies before completing the first birth
anniversary. Child survival appears to play a major role in
the acceptance and continuation of contraception (Mauldin
W.P and S.J Segal, 1988). In this chapter, we have identified
the factors influencing the current use of contraception during
fertility transition in Bangladesh.
The determinants of contraceptive
use are important in any effort to reduce fertility within
a country. Caldwell and Caldwell (1987) pointed out that the
path of fertility will be determined by the extent to which
contraception substitutes abstinence, and ultimately by the
extent to which it is more efficient than periodical abstinence
as a means of fertility regulation.
Several studies have been carried
out to investigate factors influencing the use of contraceptives.
In Bangladesh such studies include that of Shahid and Chakraborty
(1989), who used multivariate logistic regression technique
to examine 15 socio-economic and demographic variables and
assessed their relative importance in relation to contraceptive
use. In another study, Kabir (1990) used the Bangladesh Fertility
Survey in 1989 and the Bangladesh Demographic and Health Surveys
(BDHS) during 1993-94 and 1996-97 to investigate the determinants
of contraceptive use among the currently married women under
50 years of age. Bi-variate analyses were used to assess the
differentials and multivariate analysis used to find the determinants
of the current contraceptive use.
The major focus of the following
sections is the examination of the extent of contraceptive
use. This chapter examines the individual-level factors related
to contraceptive use only.
Data Collection
and Methodology
Data
The data was collected from a field survey conducted
in the district of Rajshahi of Bangladesh under the project
of UNFPA entitled "Strengthening the Department of Population
Science and Human Resource Development". These data were
collected from both rural and urban areas of Rajshahi district.
Information was collected from 2000 ever-married women by
interview method. Respondents were selected by purposive sampling
method. For rural areas we had selected Baksimoil union of
Mohanpur thana and for urban areas we have selected 3 wards
of Rajshahi Metropolitan city corporation.
Methodology
Percentage distribution and the average value are used
to investigate the overview picture of the respondents for
some selected socio-demographic characteristics.
Data analytic method envisaged in this paper is percentage
distribution and logistic regression analysis. In logistic
regression, just as linear regression, the codes for the independent
variables must be meaningful. We must decode the values of
the independent variables by creating a new set of variables
that correspond, in some way, to the original categories.
When we have a variance with more than two categories, we
must create a new variable to represent the categories. The
number of new variables required to represent a categorical
variable is one less than the number of categories. For example,
if instead of the actual values for education of the respondents,
we had values of 0, 1 depending on whether the value was `no
education`, and `some education`. The value ``no education``
would be represented by codes of 0 and it is called reference
category. If we use indicator variables for coding, the coefficient
for the new variables represent the effect of each category
compared to a reference category. The coefficient for `some
education` is the change in log odds when the lower primary
is compared to no education. The coefficients for no education
are necessarily zero, since it does not differ from itself.
The logistic regression procedure will automatically create
new variables for categorical variables.
Current Use of Contraception
Women, at the time of the interview, were asked if they were
currently doing something or using a method to delay or to
avoid getting pregnant. This information is very useful as
a measure of one of the proximate determinants of fertility
as well as a measure of the coverage of family planning programmes
(Bertrand et al., 1993). We computed contraceptive prevalence
(the percentage of all married women currently using some
type of contraception) according to their background characteristics.
The percentages of results are presented in Table 1. The table
shows that 69.4 percent of the married women were using contraception
at the time of the interview.
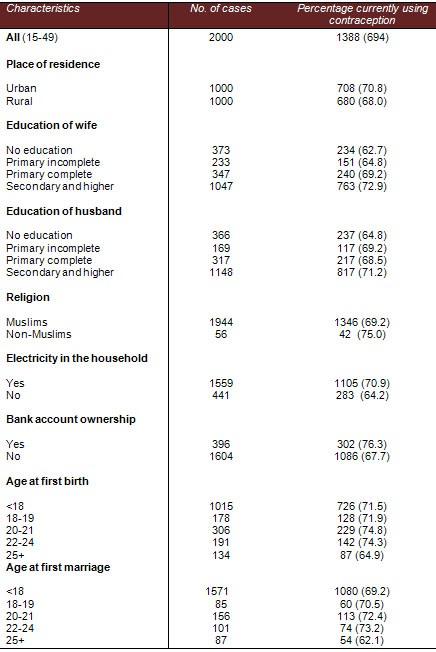
Table 1: Percentage distribution of women currently using
contraceptive methods by selected background variables
(Part 1)
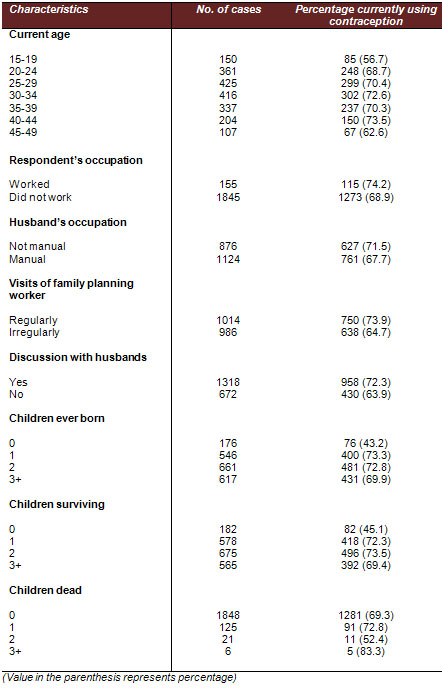
Table 1: Percentage distribution of women currently using
contraceptive methods by selected background variables
(Part 2)
Table 1 reveals that women residing
in urban areas have a contraceptive prevalence of about 3.0
percentage points higher than those residing in rural areas.
The highest prevalence is observed for women who had their
first birth and marriage above the age of 18. It is also interesting
to note that women who had their first marriage and birth
below the age of 18 years have a low percentage of contraceptive
use. However, this might reflect the interaction between early
child bearing and no usage of contraception as low contraceptive
prevalence leads to earlier birth.
Let us take a look at women's educational
level, which is cited as the most important variable associated
with contraceptive use in many countries. It has been observed
that better educated women are more likely to use contraception
(Rutenberg, N., M. Ayad, L.H. Ochoa, and M. Wilkinson (1999)).
The percentage of women using contraception increases consistently
with the level of education. The gap between users who attended
at least secondary school and those who never attended any
type of schooling is enormous (10.2 percentage points). This
is somehow also true when the education of their life partners
is considered.
Religious differentials in contraceptive
use have been confirmed in many societies. With regard to
religion, Non-Muslims (75.0 percent) have higher contraceptive
use than Muslim women (69.2 percent). In Muslim culture, people
believe that God has control over the human reproductive system
or that children are a gift from God. Therefore, they should
not prevent a child from coming into the world (Omari,1989).
Most women with Islamic faiths are likely to advocate this
ideology.
It is observed that women who have
electricity in their house tend to have higher contraceptive
use rate than those who reported no electricity in their house.
This may be due to the fact that electricity is itself an
indicator of modernization and may be useful for motivating
and familiarization of wives and husbands about the current
use of contraception. It is also observed from Table 1 that
current use rate is higher among women who have bank account
ownership (76.3 percent) than those who did not have bank
account ownership (67.7 percent). This may due to the fact
that women having bank accounts are more aware.
Contraceptive use is higher among women aged 40-44 years than
among women either younger or older than that. Figure 1 presents
the contraceptive prevalence by five-year age groups of women.
Contraceptive prevalence is lowest for the age group 15-19,
increases gradually to reach a maximum at the age group 40-44,
after which it decreases consistently to the age group 45-49.
The reason of such findings may be due to the fact that younger
women are seeking children but the women with edged reproductive
span (40-44) might have their desired number of children.
Thereafter, some women in the age group 45-49 might have faced
menopause and so the contraception-using rate is decreased
dramatically.
Contraceptive use rate increase with
visits of family planning workers, indicating a positive relationship
between family planning workers' visits to the couple's house
and contraceptive use. The use rate is considerable higher
(about 73.9 percent) for those respondents where family-planning
workers visit their homes regularly. Again among the women
who have discussed family planning with their husbands are
more likely to use contraception.
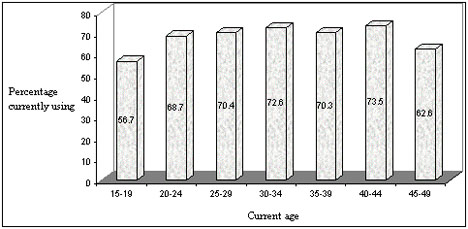
Figure 1: Percentage distribution of women currently using
contraception by current age.
Working status of women is often considered to be a determining
factor of contraceptive use. The result demonstrates that
working women are more likely to currently use contraception
compared to those who do not. The obtained results divulge
that the contraceptive use rate is the highest among those
whose husbands are not manual workers (Serviceman, businesses
man, and others).
Finally, it is important to examine
the association between the number of surviving children to
a woman and contraceptive use. The number of living children
to a woman has been found to be associated with the use of
contraception (Rutenberg et al., 1991;Robey et al., 1992).
The result shows that women who have no living children are
less likely to use any method. The use rate increases to a
maximum of 73.5 percent for those women with 2 living children
and then declined to 72.3 percent for those having 1 living
child.
Contraceptive Method Mix
It is important to examine the specific contraceptive
methods used, since different methods have different implications
for family planning programmes. Table 2 presents the percentage
distribution of women using contraception at the time of the
interview according to the method they used and their place
of residence. It seems that most women both in rural and urban
areas use modern methods more frequently than traditional
methods. According to this table 62.7 percent women use modern
methods and an additional 6.8 percent used traditional methods,
for a total of 69.4 percent of women who used any contraceptive
methods. Notably, use of traditional methods is higher in
urban areas (7.8 percent) than in rural areas (5.7 percent).
Urban contraceptive use exceeds rural use, with 70.8 percent
of urban women using contraception compared to 68.0 percent
of rural women. Contraceptive use is almost 3.0 percentage
points higher in urban areas than in rural areas.
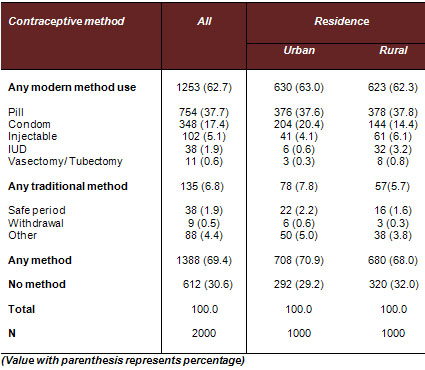
Table 2: Percentage distribution of women currently using
a contraceptive method according to the methods used and their
place of residence
The pill is the most popular method for women in urban areas
(37.6 percent) followed by condoms (20.4 percent). For women
in rural areas all three methods i.e. pill (37.8 percent),
condom (14.4 percent) and injection (6.1 percent) are popular.
In general, the pill is the most popular followed by condoms.
Several factors may account for the demanding popularity of
the pill; the single most significant benefit of the pill
is its almost 100 percent effectiveness in preventing pregnancy
and thereby removing anxiety about the risk of unplanned pregnancy.
Apart from this, the pill has a number of non-contraceptive
benefits and is quite easy to obtain.
Injectable contraceptives are popular
in rural areas due to the fact that they can be used without
the agreement of the husband or partner. Many men in rural
areas do not want their sexual partner to use any contraceptives
methods. Men would like many children as a future labor force
or future social security.
Contraceptive Use in Relation to Self-reputed Need
In this section, fertility preferences and contraceptive use
are discussed jointly to analyze contraception in relation
to need, namely the desire among women to avoid future childbearing
altogether.
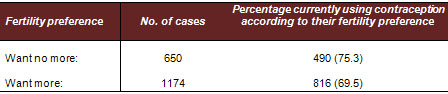
Table 3: Percentage of women using contraception according
to their fertility preference
Table 3 shows the relationship between
contraceptive use and self-reported desire to limit family
size. The entire analysis is done for those women who have
at least one surviving child. Among the women, who said they
wanted no more children, only 75.3 per cent were practicing
contraception. This compares to a figure of 69.5 per cent
for those who said they wanted another child at some time
in the future. Thus, "limiters" and "spacers"
were found to be quite close to contraceptives users.
Multivariate Analysis of the Determinants
of Current Contraceptive Use
Binary logistic regression is the multivariate analysis technique
used to predict the presence or absence of a characteristic
or outcome based on values of a set of predictor variables.
It is similar to linear regression model but is suited to
models where the dependent variables are dichotomous. In this
section, logistic regression will be used to examine the relative
importance of the determinants of contraceptive use. The response
variable is used or non-use of contraceptives at the time
of the survey. Table 1 describes the data used for the multivariate
analysis.
Results of Logistic Regression
Analysis
Table 4 presents the model for the determinants of current
contraceptive use for women. Nine variables were found to
influence the use of contraceptives significantly. The analysis
indicates that women's education is the strongest predictor
of the use of contraceptives. Women with 'incomplete primary'
education were 1.03 times more likely to use contraceptives
than women who had no education. The likelihood of using contraceptives
increases further as the educational level increases beyond
'lower primary'. Women who had at least secondary and higher
education, were 2.13 times more likely to use contraceptives
than women without education. It is interesting to note that
the education of a woman's partner has also impact independently
of her own educational level. The direction of this effect
is the same, although the odds ratio is weaker. The fact that
both the education of women and of their partners was significant
indicates that these two variables have separate effects in
determining contraceptive use. The prevalence of contraception
depends to a large extent on the type of the place of residence.
Women residing in rural areas are 0.79 times less likely to
use contraception than their counterparts residing in urban
areas.
Non-Muslim women are 1.36 times more
likely to use contraceptives than MuslIm women. It seems that
those respondents who have electricity in their house were
1.20 times more likely to use contraception than those respondents
who have not electricity in their houses. It seems that respondents
who have bank account ownership were 1.29 times more likely
to use contraception than those who have not, which may be
due to the awareness of these women.
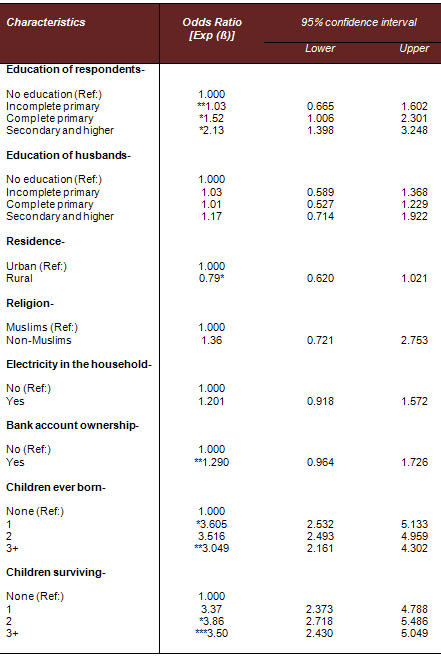
Table 4: Odds ratio associated with the determinants of current
contraceptive use for married women (Part 1)
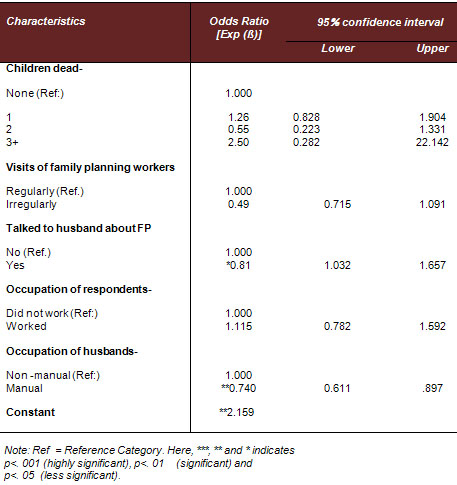
Table 4: Odds ratio associated with the determinants of
current contraceptive use for married women (Part 2)
Again, the number of living children
influences the use of contraception. Women with 1 child are
3.37 times more likely to use contraceptives than women without
surviving children and women with 2 children are 3.86 times
more likely to use contraceptives than women without surviving
children. Women with 3 and more surviving children are 3.50
times more likely to use contraceptives than women without
any surviving child. Women with one child were less likely
to use contraception, while the chance of using a method increased
as a woman's family becomes bigger than two children. Further
occupation of husbands is found to have significant effect
on contraception use. Respondents whose husbands are manual
workers have 0.74 times less use of contraception that those
whose husbands are not manual workers.
From the results of logistic regression
analysis it also appears that those respondents where family
planning workers do not visit their houses are 0.49 times
less likely to use contraception than those where FP workers
visit their house. In view of the likelihood that the visits
of family planning workers can motivate the women by counseling
on family planning methods and disseminating family planning
services and supplies to achieve their widespread availability.
Talking to husband about FP has also a net effect on current
use of contraception. Among the women who have not discussed
FP with their husbands they are 0.81 times more likely to
use contraception than those who have discussed FP.
Although, age at first birth did
not show any significance (Table 5), age at first marriage,
and current age are highly related to contraceptive use. Women
who had first marriage between age 18 and 19 were 1.23 times
more likely to use contraceptives than those who had the same
experience below age 18. The odds ratio increases as the age
at first marriage rises. This shows that women who marry at
an early age do not do something to plan their families. This
was also found in bivariate analysis done earlier.
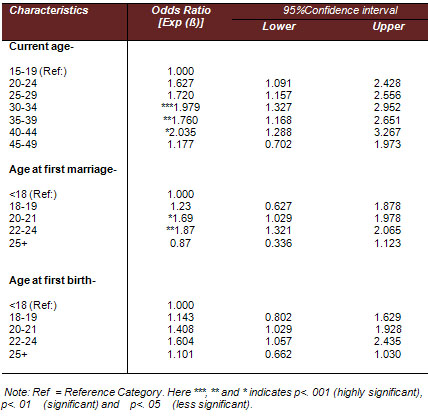
Table 5: Odds ratio associated with the retrospective determinants1
of current contraceptive use for women.
Conclusions
and Policy Implications
In this study a limited attempt has
been made to investigate some important aspects of contraceptive
behavior among married women of our study area. The analysis
shows that, use of contraception is low in our study area.
According to survey data, the percentages of women aged 15-49
currently using any method is 69.4 respectively. Methods most
widely used are the pill and condom. The common traditional
methods are periodic abstinence and withdrawal. Notably, use
of traditional methods is higher in urban areas, which suggests
some Bangladeshi couples may be discriminating in their choice
of traditional methods. However, in general the main reasons
for not using contraceptives among women may be attributed
to several socio-economic and cultural factors, such as education,
religiosity, social conservativeness, husband-wife communication,
occupation, economic condition, including a need for more
children, and opposition by the respondent to contraception.
Among the factors determining contraceptive use among women,
education appears to be the most significant; education is
positively associated with contraceptive use. Evidence suggests
that education not only increases awareness of social mobility
and creates a new outlook and rationalism among couples, but
also reduces desired family size by raising desired living
standards, bringing about a better understanding of the reproductive
process, better knowledge about health care and access to
modern and effective means of birth control. The region of
residence, occupation of husband and bank account ownership,
visits of family planning workers and talking to husbands
about family planning also appear to be significant factors
determining the level of contraceptive use among the women.
A multivariate analysis of the determinants of current contraceptive
use among women showed that for women, 9 out of 16 variables
chosen influenced the use of contraception significantly.
Women residing in rural areas, with no education, no bank
account ownership, married below age 18 or without a living
child, and not discussing FP with their husbands, are less
likely to use contraception than other women.
In the light of the above discussions there are clear policy
and programmatic implications. Any further acceleration in
contraceptive prevalence and fertility decline will require
major efforts directed at improving women's status, increasing
access to the media and improving programme efforts in the
low performing divisions especially in rural areas. The government
of Bangladesh should aim not only at consolidating the level
of success it has already achieved in family planning a part
of the broader reproductive health service package. Priority
should also be given to development in the social sector,
including enhancement of women's status, especially through
increased female educational and employment opportunities,
and an improvement in access to media. Such investments, in
addition to their direct benefits, would further accelerate
the process of rising use of contraception and further the
process of fertility decline in the country.
1. Retrospective determinants: Demographic
events that occurred in a given past period, generally terminating
at the time of the survey
References
Bertrand, J.T., E.K. Bauni, R.J.
Lesthaeghe, M.R. Montgomery, O. Tambashe, and M.J. Wawer (1993).
Factors Affecting Contraceptive Use in Sub-Saharan Africa.
Washington D.C.: National Academy Press.
Bongaarts, J. (1991): The KAP-Gap and the Unmet Need for Contraception.
Population and Development Review, 17(2):293-313.
BDHS (1999-2000). Bangladesh Demographic and Health Survey,
1999-2000. National Institute of Population Research and Training.
Dhaka, Bangladesh. Mitra Associates and Macro international
Inc. Calverton. Maryland, USA, 1999.
Courtis, S. (1993). The Impact of Postpartum Redundant Use
of Contraception of Contraceptive Failure Rates. Paper presented
at the Population association of American Conference, May,
5-7, 1994.
Caldwell, J. and P. Caldwell (1987). The Cultural Context
of High Fertility in Sub-Saharan Africa. Population and Development
Review, 13(3):409-437.
Duza, Badrud and M. Nag. (1993). High Contraceptive Prevalence
in Matalb, Bangladesh: Underlying Processes and Implications,
in R. Leete and I. Alam (eds). The Revolution in Asian fertility:
Dimensions, Causes and Implications, Oxford:Carelona Press.
Khuda, B.J. Stoeckel and N. Piet-Pelon. (1997). The Bangladesh
Family planning Program: Learned and Directions for the Future.
Dhaka International Center for Diarrhoeal Disease Research,
Bangladesh ICDDRB, monograph, 6.
Kabir M and A. K. Obidur Rab (1990). Fertility and its Proximate
Determinants. South Asia Study of Population Policy and Programmes
Bangladesh UNFPA Dhaka
Mauldin, W.P. and S.J. Segal(1988). Prevalence of Contraceptive
Use: Trends and Issues. Studies in Family Planning, 19(6)335-353.
Omari, C.K. (1989). Socio-cultural Factors in Modern Family
Planning Methods in Tanzania. Lewinston, NY, U.S.A.: The Edwin
Mellen Press.
Rutenberg, N., M. Ayad, L.H. Ochoa, and M. Wilkinson (1991):
Knowledge and Use of Contraception. Demographic and Health
Surveys Comparative Studies No. 6, Columbia, Maryland, USA:
Institute for Resource Development/Macro International Inc.
Ullah and Chakraborty. (1993). Socio-Cultural Factors Affecting
Practice of Contraception in Metropolitan Urban Areas of Bangladesh.
Paper presented at the seminar of Fertility of Bangladesh
held at Coxe's Bazar, p.op.21-23
Ross, J.A. and E. Frankenberg (1993): Findings from Two Decades
of Family Planning Research. Population Council, New York.
Rutenberg, N., M. Ayad, L.H. Ochoa, and M. Wilkinson (1991):
Knowledge and Use of Contraception. Demographic and Health
Surveys Comparative Studies No. 6, Columbia, Maryland, USA:
Institute for Resource Development/Macro International Inc.
Shahidullah, M. and N. Chakraborty (1989). Factors Affecting
Use of Contraception in Bangladesh: A Multivariate Analysis.
Department of Statistics, University of Dhaka-1000, Bangladesh
Ullah and Chakraborty. (1993). Socio-Cultural Factors Affecting
Practice of Contraception in Metropolitan Urban Areas of Bangladesh.
Paper presented at the seminar of Fertility of Bangladesh
held at Coxe's Bazar, p.op.21-23
|
 |

