| |
November
2014
- Volume 8, Issue 4
Moving
toward Integration: Group Dance/movement therapy with children
in Anger and Anxiety

|
 ( (
|
Anahita Khodabakhshi Koolaee
(1)
Mehrnoosh Sabzian (2)
Davood Tagvaee (3)
(1) Department of counseling,
Islamic Azad university,
Science and Research branch of Arak, Arak, Iran
(2) Department of psychology, Islamic Azad university,
Science and Research branch of Arak, Arak, Iran
(3) Department of psychology, Islamic Azad university,
Science and Research branch of Arak, Arak, Iran
Correspondence:
Anahita Khodabakhshi Koolaee
Department of counseling,
Islamic Azad university,
Science and Research branch of Arak, Arak, Iran
Email: anna_khodabakhshi@yahoo.com
|
|
|
Abstract
Background: Dance/ movement therapy (DMT) is
defined as the "psychotherapeutic use of movement
as a process that furthers the individual's emotional,
cognitive, social, and physical integration'. DMT can
elicit positive change, growth, and health among adults
and children.
Objective: The purpose of this study was to examine
the effect of Dance/Movement Therapy (DMT) in decreasing
levels of aggression and anxiety among children ages
6-7 years old enrolled at four private pre-school centers
in Tehran, Iran in 2013.
Method: The design of this study was Quasi-experimental
pre-post test with control group. Thirty children were
selected by random method from four private pre-schools
in Tehran. Then, 15 children were randomly assigned
to the experimental group and 15 other children were
elected for the control group. The dependent variables,
aggression, and anxiety were measured twice throughout
the 10-week study. Ten one-hour group DMT sessions were
given as the interventions for the experimental group.
For gathering data we used Children's Inventory of Anger
(ChIA) and Spence Children's Anxiety Scale (SCAS). Data
was analyzed by Analysis of Covariance (ANCOVA).
Results: There was a significant difference in
aggression and anxiety scores between the two groups
of participants. The experimental group showed lower
incidence aggression and anxiety after DMT intervention.
Conclusion: The findings of this research suggest
DMT can be beneficial for all children with Anger and
Anxiety. In addition, DMT can provide a sense of safety,
self-awareness, other or people mindfulness, and mental
health for children.
Key words: Dance/movement Therapy (DMT), Aggression,
Anxiety, Pre-school children
|
Background
The American Dance Therapy Association defines dance/movement
therapy as the "psychotherapeutic use of movement to
further the emotional, cognitive, physical, and social integration
of the individual" (1). American Dance Movement therapy
points out the benefits of DMT as "There is a variety
of goals and techniques and activities used in individual
and group DMT sessions, including; movement behavior, Expressive,
communicative, and adaptive behaviors are all considered for
group and individual treatment. Body movement, as the core
component of dance, simultaneously provides the means of assessment
and the mode of intervention for dance/movement therapy. DMT
is useful for mental health, rehabilitation, medical, educational,
and forensic settings, and in nursing homes, day care centers,
disease prevention, health promotion programs and in private
practice. DMT is effective for individuals with developmental,
medical, social, physical, and psychological impairments.
In addition, DMT is used with people of all ages, races, and
ethnic backgrounds in individual, couples, family, and group
therapy formats"(1). Schmais (1985) looked at factors
within group dance/movement therapy that elicit positive change,
growth, and health in its participants. Factors that can be
seen in typical group dance therapy sessions include synchrony,
expression, rhythm, vitalization, integration, group cohesion,
education, and symbolism (2). There have been bodies of researches
done to examine the effects of Dance/ Movement therapy for
children. For example, Leventhal discussed DMT for the special
needs child. DMT could be beneficial indirectly for Special
children and create a new chance for them to learn new skills
and modify their patterned behaviors (3). In addition, Shennum
(1987) found out that the children who received DMT sessions
had lower levels of emotional unresponsiveness and negative
acting out (4). Throughout the literature review there have
been implications that Dance/Movement Therapy (DMT) has an
impact on mental health of children who present with various
issues, including severe trauma (5), depression, attention
deficit hyperactive disorder (ADHD), conduct disorder, as
well as psychosis, anxiety, and post-traumatic stress resulting
from physical and sexual abuse (6 & 7). DMT was also found
to have impact on children in struggle with communication
and motor skills ( 8), victims and children who were soldiers
and torture survivors (9 & 10). DMT education for clinical
staff examined by Lundy & McGuffin (11) has been shown
to have a positive effect on therapeutic holding with children
in an in-patient setting. Capello argues the effect of dance/movement
therapy in reviews of cross-cultural study by literature;
the literature implies it has influenced children's development
issues surrounding differences in child rearing and children
who have been survivors of war and torture (12).
Dance/Movement Therapy has been used as a tool to address
aggression and empathy; the curriculums have been utilized
in public schools as a preventative measure (13 & 14),
in a multi-cultural school setting (15), and in a residential
treatment program for emotionally and behaviorally disturbed
children with histories of abuse and/or neglect (4).
In some countries around the world, dance/movement therapy
brings a new opportunity for therapeutic and education methods
for clinicians and staff (Capello, 2008). In Iran Dance/Movement
Therapy is not approved as a formal therapeutic adjunct or
the curriculum in school settings. While, in Iran some private
pre-schools are using DMT for helping children with hyperactive
behaviors.
Objective
In this study, we examine the effect of Dance/ Movement Therapy
(DMT) as a new adjunctive therapy to help children with aggression
and anxiety in Tehran in2013.
Method
1. Participants and plan:
The design of this study was Quasi-experimental pre-post test
with control group. Thirty (6-7years old) children were selected
by random method from four private pre-schools in Tehran by
2013. Then, 15 children were randomly assigned to the experimental
group and 15 children were elected for the control group.
The dependent variables, aggression, and anxiety were measured
twice throughout the 10-week study. Ten one-hour group DMT
sessions were given as the interventions to the experimental
group. The DMT sessions were described in Table 1.
Table 1: Dance/movement therapy sessions
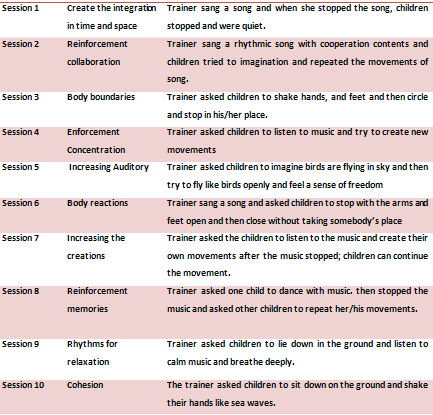
• Trainer ended every session with snacks and talking
about the session.
• All sessions were performed by Dance/Movement trainer.
For Children to be eligible for this study they must
1) Have been between the ages of 6-7 years old
2) Have been identified by their primary therapist
to address continuous serious aggressive behaviors and anxiety
3) They have not suffered severe physical disability
4) Carry a diagnosis of at least one of the following:
Attention Deficit Hyperactive Disorder (ADHD), Oppositional
Defiant Disorder (ODD), Anxiety Disorder, or Learning Disorder
NOS
5) They have normal IQ
6) Be assigned to the identified pre-school centers
in Tehran
Subject Exclusion Criteria
Children may not be enrolled in this study if they
1) Were not enrolled at the identified pre-schools
2) Were not assigned to the designated classroom
3) Were younger than 6 years old or older than 7 years
old at any time from the onset of the study to the end of
data collection.
4) Carried a diagnosis on the Autism spectrum, Pervasive
Developmental Disorder (Asperger's Syndrome, Childhood Disintegrative
Disorder, or Rett's Syndrome), or Mental Retardation may not
participate in the study.
5) They suffered severe physical disability.
2. Measurement:
Participants responded to two questionnaires including; Children's
Inventory of Anger (ChIA), and Spence Children Anxiety Scale
(SCAS).
Children Inventory of Anger (ChIA):
The Children's Inventory of Anger is a 40-item child self-report
rated from 1 (no anger) to 4 (extreme anger) for children
6-16 years old. This questionnaire made by Nelson and Finch
(1993) and was reviewed in 2000. Children are asked to evaluate
their response to potentially provoking events (e.g, ''someone
cuts in front of you in a lunch line''). Although the Children's
Inventory of Anger has not been used in studies of parent
management training, it has demonstrated sensitivity to change
in psychosocial interventions with children (Nelson and finch,
2000). The ChIA includes subtests and scores in the following
areas: Frustration, Physical Aggression, Peer Relationships,
Authority Relations, and Inconsistent Responding Validity
Index. The test-retest reliability was Pearson's product-moment
correlation coefficient (r= 0.63 to 0.90) and internal consistency
was good (a = 0.96) (16). Validity
for the measure is supported in its correlation with peer
ratings of anger (17).
In Iran Children Inventory of Anger was translated to Persian
by researchers in this study and the test-retest reliability
was Pearson's product-moment correlation coefficient (r= 0.65
to 0.75) and internal consistency was good (a
= 0.86).
Spence Children's Anxiety Scale
(SCAS):
The Spence Children's Anxiety Scale created by Spence
(1998) is a self-report measure of Anxiety originally developed
to examine anxiety symptoms in children aged 8-12 years. The
SCAS consists of 44 items, 38 of which assess specific anxiety
symptoms relating to six sub-scales, namely social phobia,
separation anxiety, panic attack/agoraphobia, obsessive-compulsive
disorder, generalized anxiety and physical injury fears. The
remaining six items serve as positive ''filler items'' in
an effort to reduce negative response bias. Respondents are
asked to indicate frequency with which each symptom occurs
on a four-point scale ranging from Never (scored 0) to Always
(scored 3). A total SCAS score was obtained by Sum scores
of the 38-anxiety symptom items. Previous studies have demonstrated
high internal consistency, high concurrent validity with other
measures of child and adolescent anxiety, and adequate test-retest
reliability for total score (r= 0.92)(18). In Iran SCAS was
translated to Persian by Mosavi et al (2007) with adequate
test-retest reliability for total score (r= 0.89) (19).
3. Procedure, statistical methods,
and code of ethics:
Participants answered all of the questionnaires independently
under supervision of interviewers and parents filled out with
informed consent.
When participants were selected, researchers were told the
aim of the study to children and their parents and asked the
children to answer the questionnaires. For filling out the
questionnaire, reviewers read the questions one by one and
marked the questionnaire, because children could read and
write independently.
The data gathered from research was analyzed by Descriptive
statistical methods including; Mean, Standard deviation, and
percent frequency. In addition, inferential statistical methods
like, Analysis of Covariance (ANCOVA) implemented for research.
Data was analyzed by SPSS statistical package version 18.
Results
Table 2, shows the difference between mean score of Children
Inventory of Anger (ChIA) overall score in the two groups
with ANCOVA. Results of the Children Inventory of Anger (ChIA)
is shown in Table 2. Dance / Movement Therapy (DMT) intervention
in the treatment group decreased the level of Anger (68.20
± 13.23 vs. 96.23 ±16.02; p=0.0001).
Table 2: Differences between mean score of Children Inventory
of Anger (ChIA) overall score in the two groups with ANCOVA
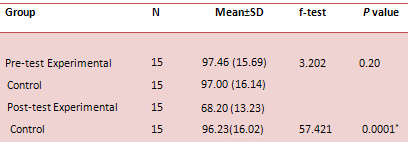
Abbreviations: SD, Standard Deviation; f, F-test
The
results showed no significant differences between the mean
ChIA in pre-test scores. Rather, differences in the mean scores
of the ChIA in the two groups were significant after intervention
(p=0.0001), as confirmed by ANCOVA (p=0.0001; Table 2).
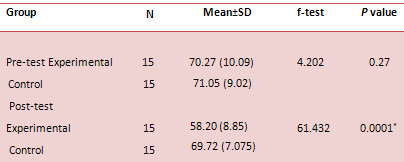
Results of the Spence Children Anxiety Scale (SCAC) presented
in Table 3. Dance / Movement Therapy (DMT) intervention in
the treatment group decreased the level of Anxiety (58.20
± 8.58 vs. 69 .72± 7.075; p=0.0001).
Table 3: Differences between mean score of Spence Children
Anxiety Scale (SCAS) overall score in the two groups with
ANCOVA
Discussion
The present research shows that Dance/Movement Therapy has
a beneficial effect in children with Anger and Anxiety. The
DMT sessions can reduce the levels of aggression among pre-school
children. This result was consistent with the previous study,
as an example; Lanzillo (14) found that DMT decreased the
level of aggression and increased the empathy in children.
In addition, Lanzillo cited that DMT could be used as curriculum
in schools to improve the social skills and empathy in children
and prevented behavioral problems in children. Furthermore,
Hervey and Kornblum (13) implemented the mixed-method of Dance/
Movement therapy for children at-risk. Results showed that
behavioral problems had dramatically reduced in children.
In addition, in 2004, Koshland and Wittaker evaluated the
peace through the Dance/ Movement therapy (DMT) program, created
by Lynn Koshland. The program was designed for violence prevention
with multi-cultural elementary school students. The results
revealed that the levels of aggression, and disruptive behaviors
had decreased, while, self-control among children who received
the DMT intervention had improved (15).
Caf, Krofic & Tacing (1997) examined the use of creative
movement and dance on children with struggles with communication
and self- awareness and expression of their feelings. They
found that the movement and dance could be helpful for children
participating in the research. Teachers reported that children
became more expressive of their feelings and more active (8).
There are several activities and modules applied in individual
and group Dance/movement therapy (DMT) sessions, including
Role-playing, the use of imaginative play, and structured
and non-structured movements (14).
As Leventhal (1980) noted Dance/ Movement Therapy (DMT) can
indirectly teach. The Children are participating in DMT activities;
they are more receptive to learning new skills and changed
their behaviors (3).
In conclusion DMT sessions can be beneficial for all ages
from children to aged people. DMT can improve positive coping
skills, impulse control, and self- esteem; bring social support
and interactions, self-awareness, improve body language, body
boundaries, in addition, to building empathy and ability to
form healthy relationships with others (14). DMT is used in
Iran as an informal program in pre-schools but researchers
suggest that DMT and Rhythmic Movements can be seen as a new
curriculum program for creating a new chance for children
to explore their own life through movements.
References
1- American Dance Therapy Association (ADTA) (2014). What
is Dance/ Movement Therapy? Retrieved July 2014 from www.ADTA.org/
About_DMT
2- Schmais, C. Healing processes in group dance therapy. American
Journal of Dance Therapy, 1985, 8(1), 17-36.
3- Leventhal, M. B. (Ed). Movement and growth: dance therapy
for the special child. 1980, New York : Center for Educational
Research.
4- Shennum, W. A. Expressive activity therapy in residential
treatment: Effects on children's behavior in the treatment
milieu. Child & Youth Care Quarterly, 1987, 16(2), 81-90.
5- Hervey, L., & Kornblum, R. An evaluation of Kornblum's
body-based violence prevention curriculum for children. The
Arts in Psychotherapy,2006, 33(2), 113-129.
6- Erfer, T., & Ziv, A. Moving toward cohesion: Group
dance/movement therapy with children in psychiatry. The Arts
in Psychotherapy, 2006, 33(3), 238-246.
7- Gronlund, E, Renck, B. & Weibull, J. Dance/movement
therapy as an alternative treatment for young boys diagnosed
as ADHD: A pilot study. American Journal of Dance Therapy,
2005, 27(2), 63-85.
8- Caf, B., Krofkic, B, & Tancig, S. Activation of hypoactive
children with creative movement and dance in primary school.
The Arts in Psychotherapy, 1997,24,(4), 355-365.
9- Harris, D.A. Pathways to embodied empathy and reconciliation
after atrocity: Former boy soldiers in a dance/movement therapy
group in Sierra Leone, Intervention, 2007, Vol 5, Nu: 3, 203-231.
10-Harris, D.A. Dance/movement therapy approaches to fostering
resilience and recovery among African adolescent torture survivors,
Torture,2007, Vol 17, Nu: 2, 134-155.
11- Lundy, H., & McGuffin, P. Using dance/movement therapy
to augment the effectiveness of therapeutic holding with children.
Journal of Child and Adolescent Psychiatric Nursing,2005,
18(3), 135-145.
12- Capello, P. Dance/movement therapy with children throughout
the world. American Journal of Dance Therapy, 2008, 30(1),
24-36.
13- Hervey, L., & Kornblum, R. An evaluation of Kornblum's
body-based violence prevention curriculum for children. The
Arts in Psychotherapy,2006, 33(2), 113-129.
14-Lanzillo, A, A. The Effect of Dance/Movement Therapy on
Incidences of Aggression and Levels of Empathy in a Private
School for Children with Emotional and Behavioral Problems,
Unpublished Master of Arts Thesis, 2009, MA in Dance/ Movement
therapy, Drexel University, Philadelphia, USA.
15- Koshland, L., & Wittaker, J. W. B. PEACE through Dance/Movement:
Evaluating a violence prevention program. American Journal
of Dance Therapy,2004, 26(2), 69-90.
16-13- Finch AJ, Saylor CF, Nelson III WM. Assessment of anger
in children. In: Prinz RJ, editor. Advances in behavioral
assessment of children and families. Volume 3. Greenwich:
JAI Press; 1987. p 235-65.
17-Finch AJ, Eastman ES. A multimethod approach to measuring
anger in children. Journal of Psychology, 1983;115:55-60.
18- Spence, S. A measure of anxiety symptoms among children.
Behavior, research and therapy, 1998, 36(5), 545-566.
19- MoSavi, R, Moradi, A.R., Farzad, V., Mahdavi Harsini,
E, Spence, S.H. Psychometric Properties of the Spence Children's
Anxiety Scale with an Iranian Sample, 2007, www.SCASwebsite.com
|
 |

